Malaria- acquired immunity
Mediated by IgG antibodies against surface proteins of sporozoite (blocking hepatocyte invasion)
Antibody-dependent cellular cytotoxicity, opsonisation for uptake, destruction by splenic macrophages, interference with PfEMP-1 mediated cytoadhearence interactions
Immunity not sterilizing, instead “disease-controlling immunity” despite presence of parasites in bloodstream
Immunity increases with age, cumulative episodes and time living in endemic area
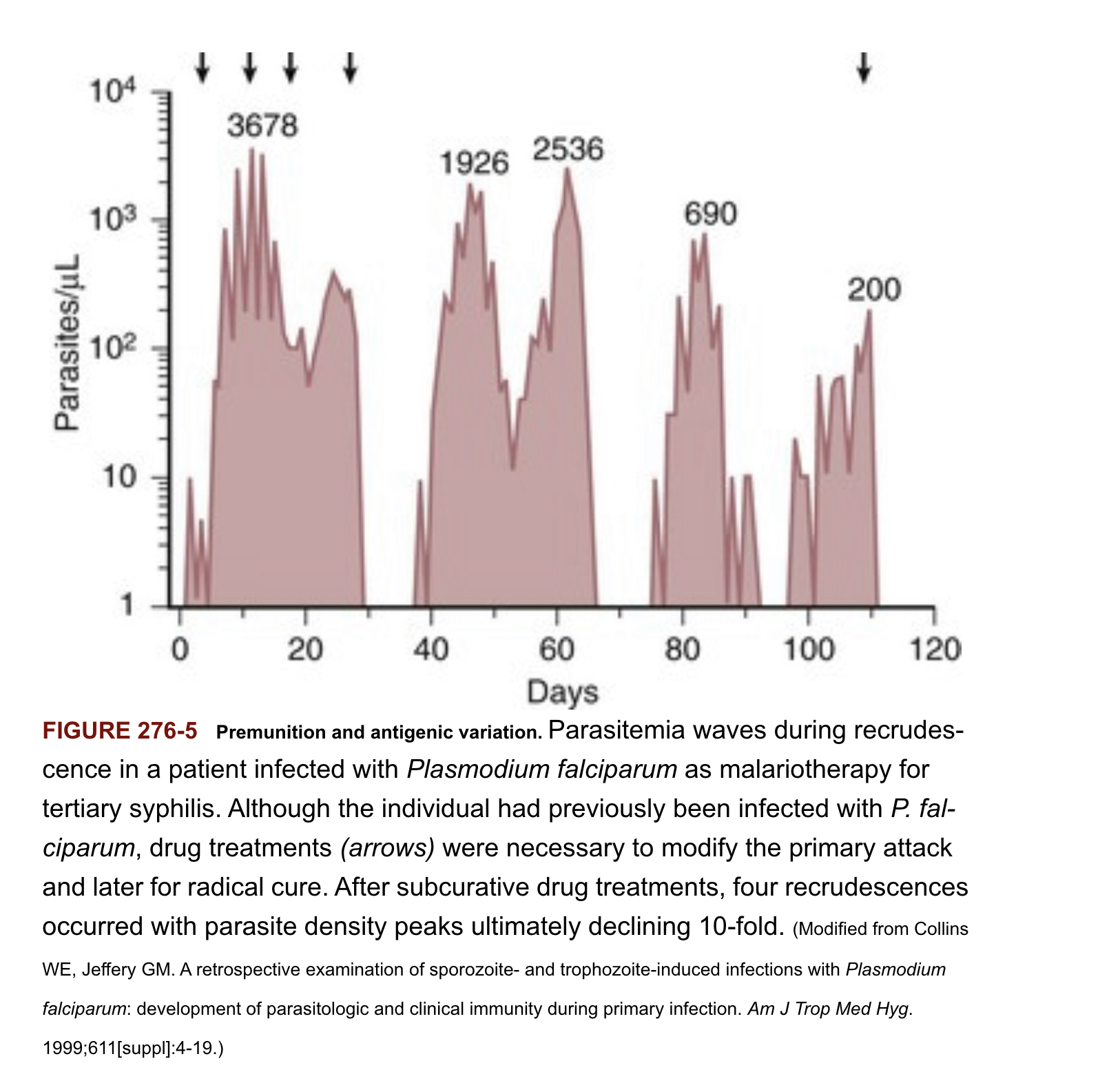
Short-lived without continued exposure to different P. falciparum variants
Antigen switching results in new waves of parasitemia, escape from antibody responses
Disease controlling immunity (premunition) after repeated infection episodes associated with development of antibody repertoire that recognizes the full spectrum PfEMP-1 variant antigens
![]()
Host traits that influence disease severity
(besides blood disorders)
Splenectomy - high parasite loads
- Splenomegaly common in malaria (removal of infected erythrocytes) but contributes to anaemia associated with disease
Pregnancy - parasites that express protein surface variant antigen 2-CSA (chondroitin sulphate-2) attaching to glycoproteins expressed in the placenta …leading to infected red blood cell sequestration in the placenta
- Increased risk of maternal and/or foetal death, miscarriage, inter-uterine growth retardation, low-birth weight, increased newborn mortality
HIV (higher degree of parasitemia, mortality)
Tuberculosis
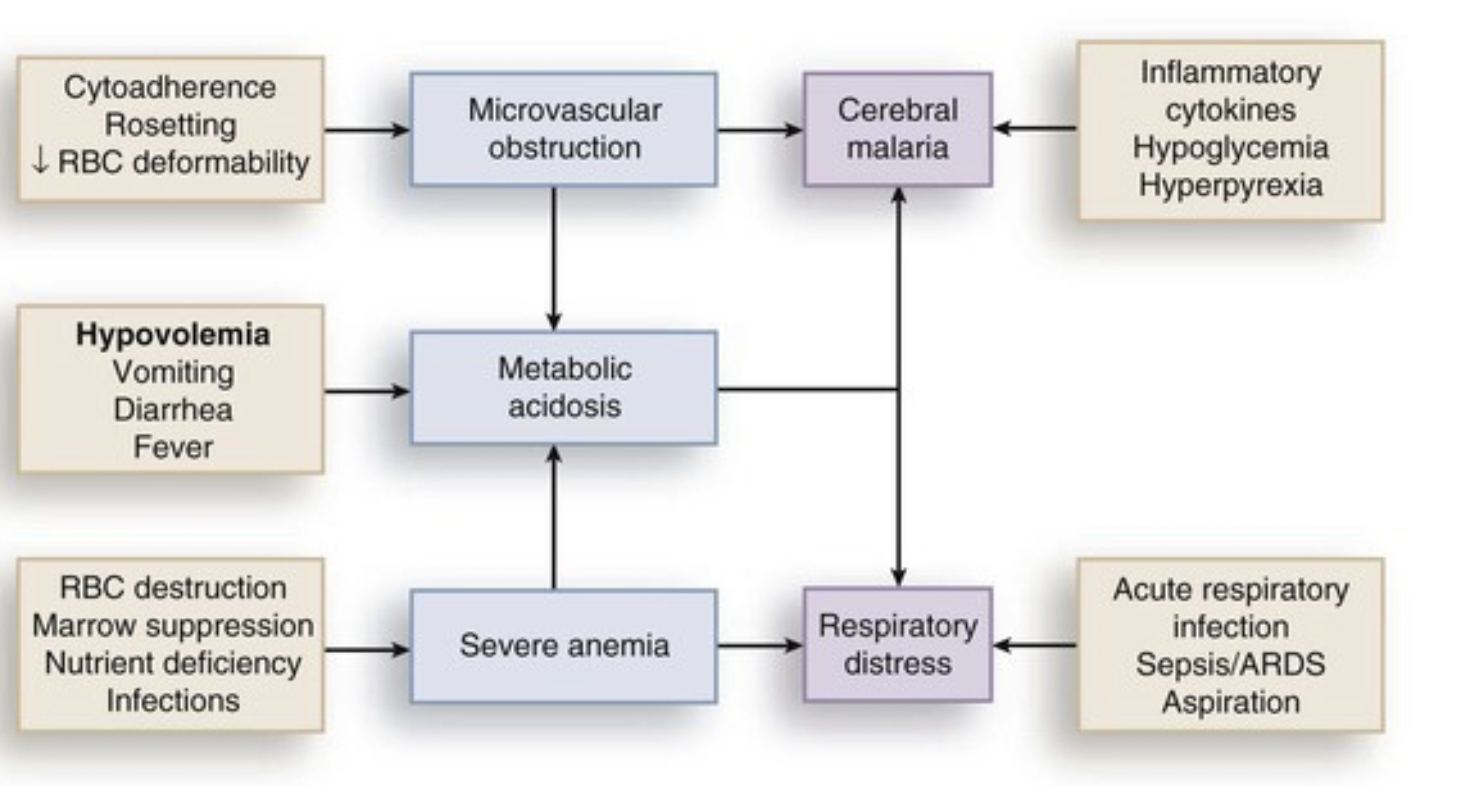
Complications of malaria
Hypoglycaemia (coma, convulsions)
Children: Impaired hepatic gluconeogenesis, increased glucose consumption in peripheral tissues and by parasites, normal insulin levels
Adults: Hyperinsulinemia due to parasite stimulation of pancreatic islet cells or quinine/quinidine therapy
Decreased food intake during prodromal period
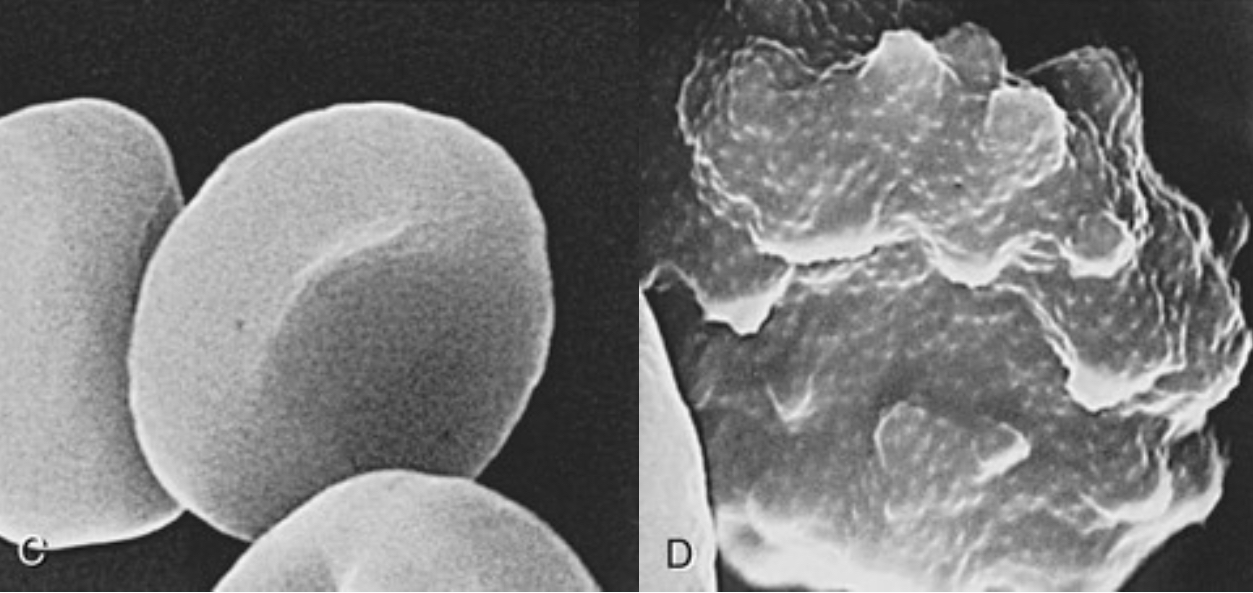
Anaemia
- Intra vascular lysis and phagocytic removal of infected erythrocytes
- TNF-α associated suppression of erythropoetin
- Normochromic, normocytic anaemia without robust reticulocyte response
Pulmonary oedema and respiratory distress
- Non-cardiogenic pulmonary oedema due to sequestration of infected erythrocytes → inflammatory response → capillary permeability → pulmonary oedema → hypoxia →acute lung injury → ARDS
- Dyspnea and increasing respiratory rate are features of impending pulmonary oedema and preclude other clinical (e.g., accessory muscle breathing) and radiologic signs (increased interstitial markings)
- TNF-α associated suppression of erythropoeitin
- Normochromic, normocytic anemia without robust reticolocyte response
Pulmonary oedema and respiratory distress
- Non-cardiogenic pulmonary oedema due to sequestration of infected erythromyctes → inflammatory response → capillary permeability → pulmonary oedema → hypoxia →acute lung injury → ARDS
- Dyspnea and increasing respiratory rate are features of impending pulmonary oedema and preclude other clinical (e.g., accessory muscle breathing) and radiologic signs (increased interstitial markings)
Metabolic (lactic) acidosis
- Reduced delivery of oxygen to tissues from combined effects of anaemia, sequesterization and hypovolemia
- Shift from aerobic to anaerobic metabolism causes lactate levels to rise
- Lactate clearance by liver reduced
Acute renal failure
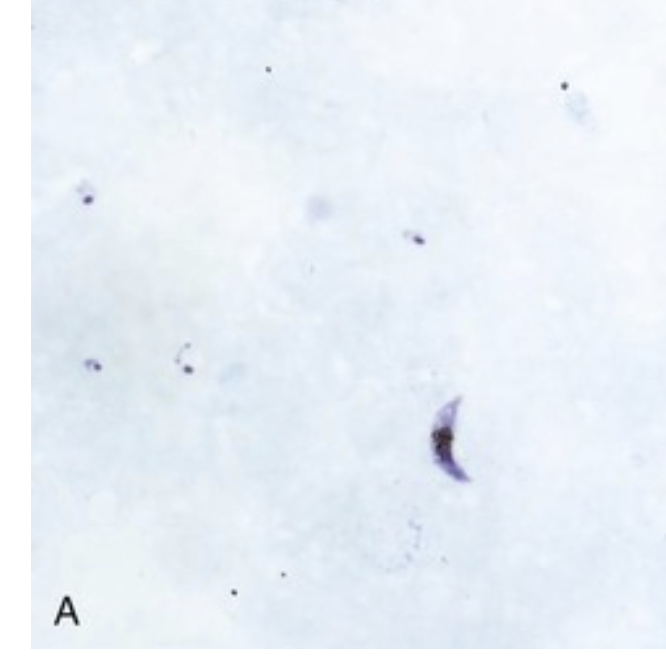
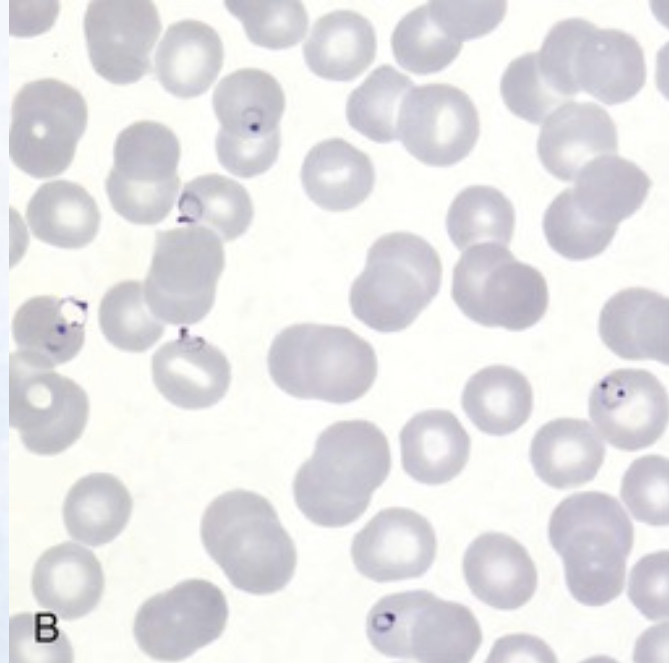
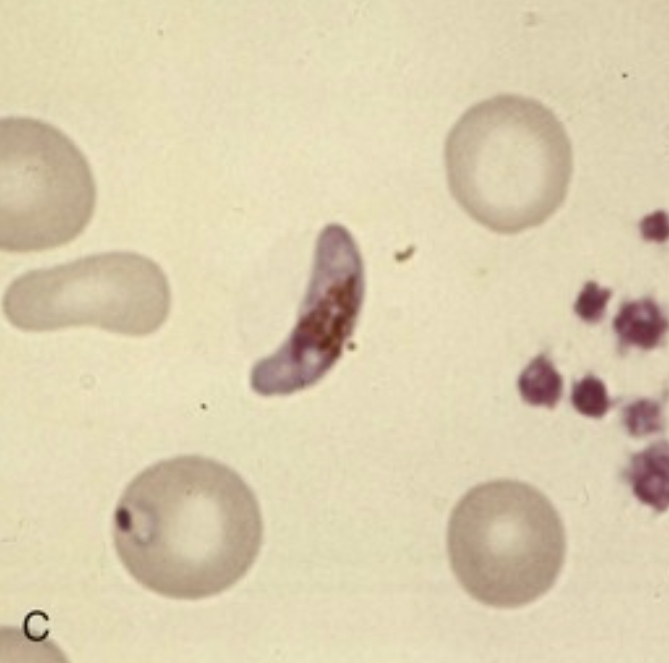
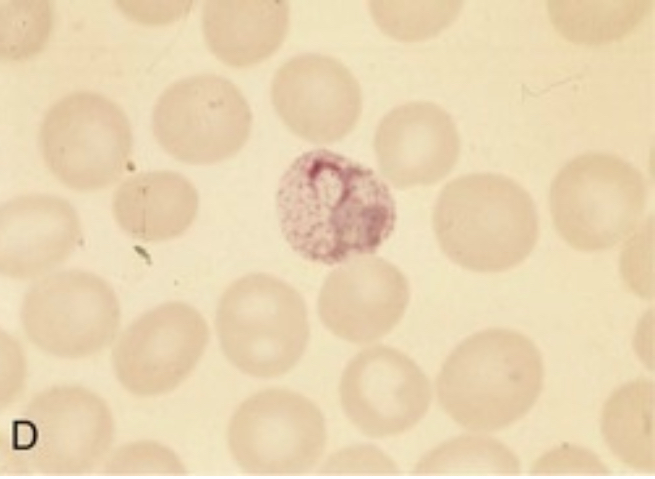
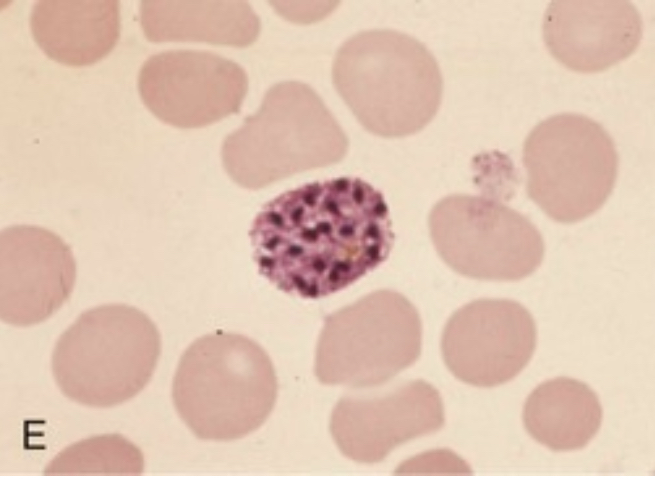
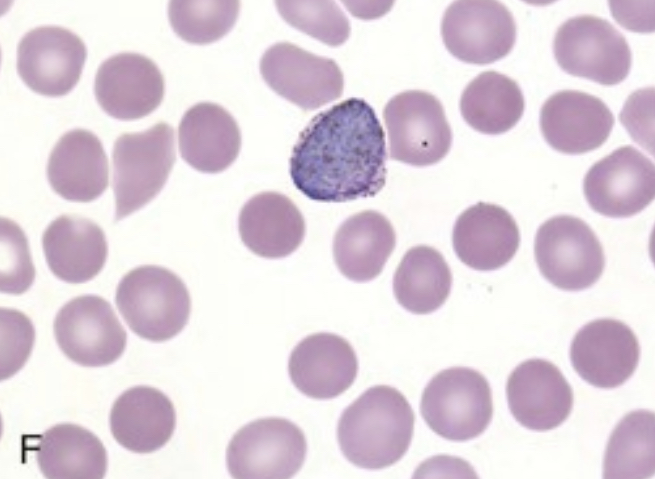
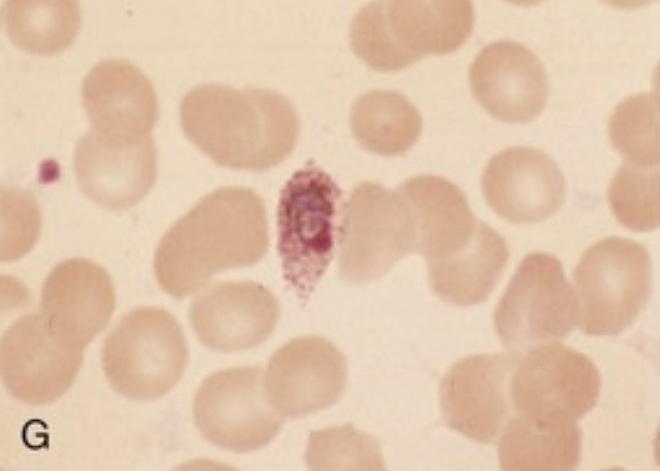
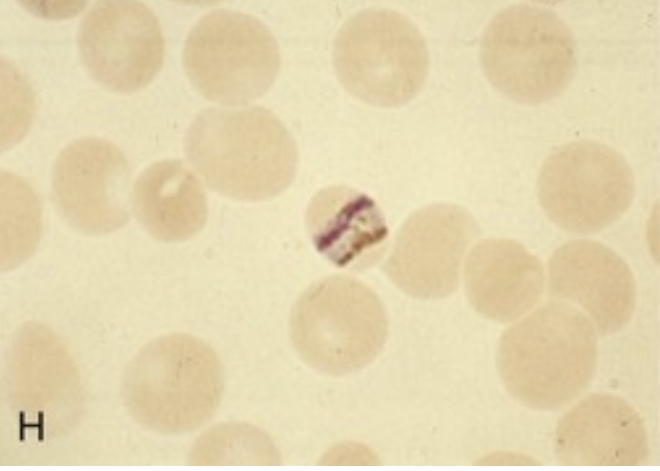
Parasites can be detected on light microscope examination of blood smear
![]()
Parasitemia
Light microscopy of Giemsa-stained blood smears is the accepted standard for diagnosis
Thick smears concentrate red cell layers 40-fold and used to screen large amounts of blood for parasites- RBCs lyse so parasites are visualized outside red cells
Parasite density can be calculated by counting the number of parasites per 200 WBCs x 40 = number of parasites per μL blood
For P. falciparum, initial blood smears may be negative because mature erythrocytes (trophozoites and schizonts are sequestered in peripheral tissues)
Smear is repeated every 12 hours until diagnosis is ruled in or ruled out
Thin smears used to determine Plasmodium species
Rapid diagnostic tests (RDTs)
Detection of Plasmodium histidine-rich protein-2 (HRP-2)
Detection of P. falciparum specific lactate dehydrogenase (LDH) and pan-Plasmodium LDH
Adequate sensitivity for P. vivax, P. ovale, and P. malaria with less sensitivity for P. falciparum
However, positive signal is proportional to P. falciparum parasitaemia, allowing for monitoring of therapeutic response
Combination tests of HRP-2/LDH under development
PCR and quantitative PCR (becoming gold standard)
- Identifies species
- Detets low levels paracetemia
- qPCR can be used to monitor therapy
- Availability in endemic areas?
Diseases with similar clinical presentations
Malaria should always fall near the top of the differential for fever in travellers or immigrants who have been in an endemic area in the previous 3 months (and remain in consideration for years afterword)
Common differential diagnosis:
Influenzae
Enteric fever
Bacteraemia/sepsis
Classic dengue fever (typically more severe myalgias , shorter incubation of 4-7 days, rash and lymphadenopathy)
Acute schistosomiasis (Katayama fever-freshwater exposure) urticaria at site of cercarial penetration (usually legs) and eosinophilia
Leptospirosis (conjunctival suffusion and rash progressing to haemorrhagic manifestations)
African tick fever (lymphadenitis, multiple inoculation eschars)
East African trypanosomiasis (sleeping sickness) -red chancre at bite site, posterior cervical lymphadenopathy, rash)
Yellow fever (conjunctival suffusion, shorter incubation period 3-6 days relative bradycardia). Unlikely in patients who have been vaccinated in last 10 years
Definition of severe malaria
| Impaired consciousness |
Glasgow coma score <11 in adults or Blantyre coma score <3 in children; inability to swallow |
| Prostration |
Generalized weakness so that a person is unable to sit, stand, or walk without assistance |
| Multiple convulsions |
More than two episodes within 24 hours |
| Acidosis |
A base deficit of >8 mEq/L, a plasma bicarbonate level of <15 mmol/L, or venous plasma lactate ≥5 mmol/L. Clinical indicators of acidosis include rapid, deep, labored breathing. |
| Hypoglycaemia |
Blood or plasma glucose <40 mg/dL (<2.2 mmol/L) for children ≥5 years and adults; blood or plasma glucose <54 mg/dL (<3 mmol/L) for children <5 years |
| Severe anaemia |
Haemoglobin concentration ≤5 g/dL or hematocrit ≤15% in children <12 years of age (<7 g/dL and <20%, respectively, in adults) with parasite count >10,000 parasites/uL |
| Renal impairment |
Plasma or serum creatinine >3 mg/dL (265 umol/L) or blood urea >20 mmol/L |
| Jaundice |
Plasma or serum bilirubin >50 umol/L (3 mg/dL) with one of the following:
- Plasmodium falciparum parasite count >2.5% parasitemia
- Plasmodium knowlesi parasite count >20,000 parasites/uL |
| Pulmonary edaema |
Radiographically confirmed or oxygen saturation <92% on room air with respiratory rate >30/minute, often with chest indrawing and crepitation on auscultation |
| Significant bleeding |
Including recurrent or prolonged bleeding (from the nose, gums, or venipuncture sites), hematemesis, or melena |
| Shock |
Compensated shock is defined as capillary refill ≥3 seconds or temperature gradient on leg (mid to proximal limb), but no hypotension. Decompensated shock is defined as systolic blood pressure <70 mmHg in children or <80 mmHg in adults, with evidence of impaired perfusion (cool peripheries or prolonged capillary refill). |
| Hyperparasitaemia |
P. falciparum:
- In non-immune travelers: parasitemia ≥5%[3]
- All patients: parasitemia >10%
P. knowlesi:
- Parasite density >100,000 parasites/uL
Plasmodium vivax:
- No established parasite density thresholds |
Therapy- General principles
P. falciparum malaria can be fatal if not diagnosed and treated promptly an appropriately
- Especially true for non-immune travellers returning from visits to malaria-endemic areas
Malaria is a disease of protean manifestations, diagnosis is delayed by non-specific clinical presentation and unimpressive normal laboratory tests- especially if blood smears (and available rapid diagnostic tests) are not examined
Life-threatening manifestation (i.e. convulsions, hypoglycaemia, pulmonary oedema) can develop rapidly in patients who appear well at presentation or respond to antimalarial drugs
Pregnant women, young children and elderly are at increased risk and should be hospitalized regardless
If patient develops malaria despite prophylaxis, they should receive a different antimalarial regimen for treatment
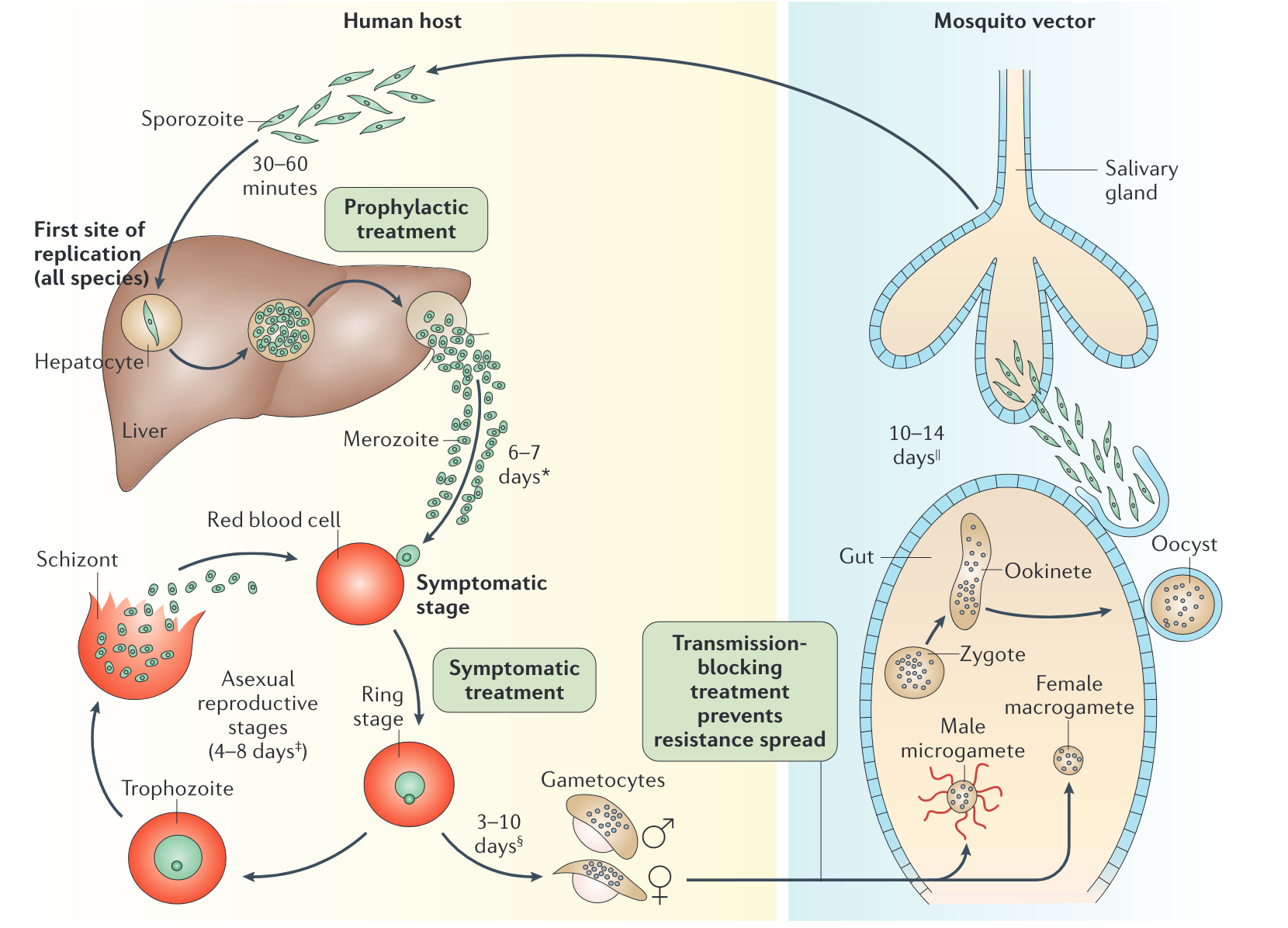
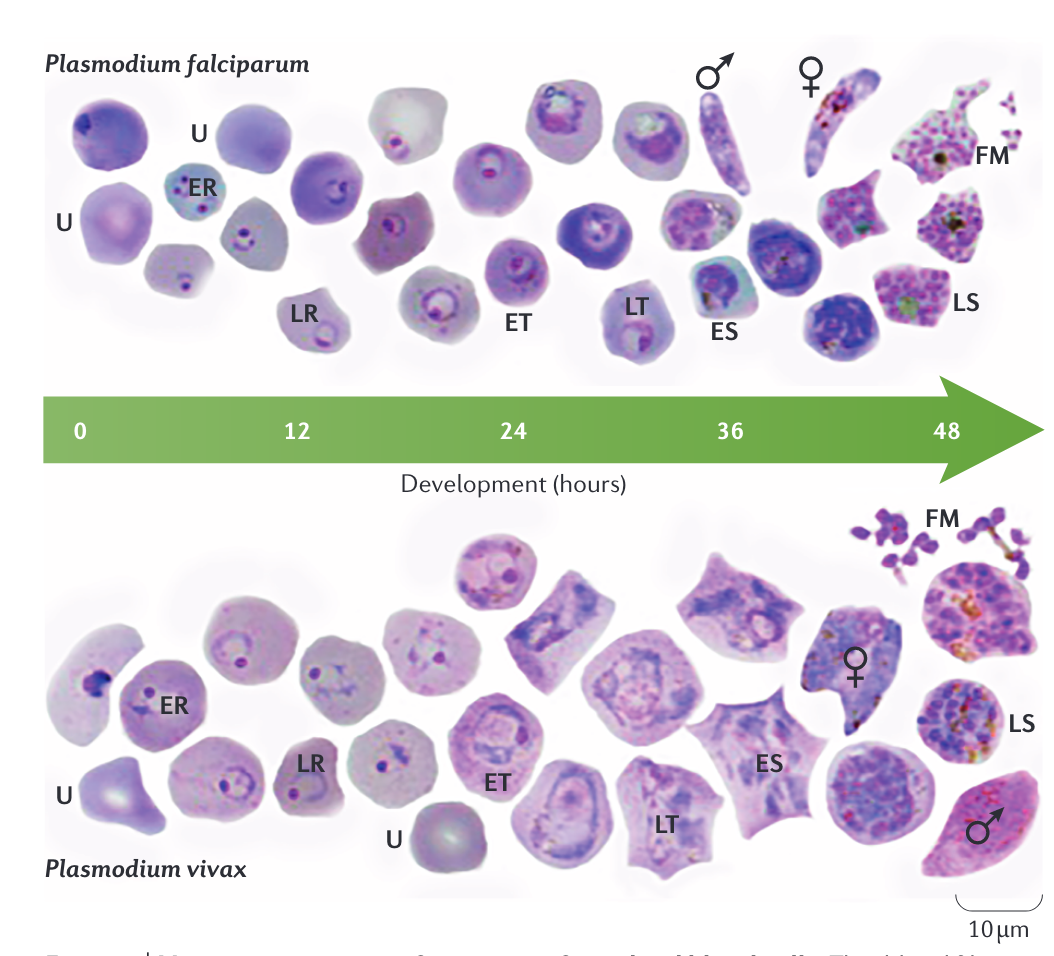
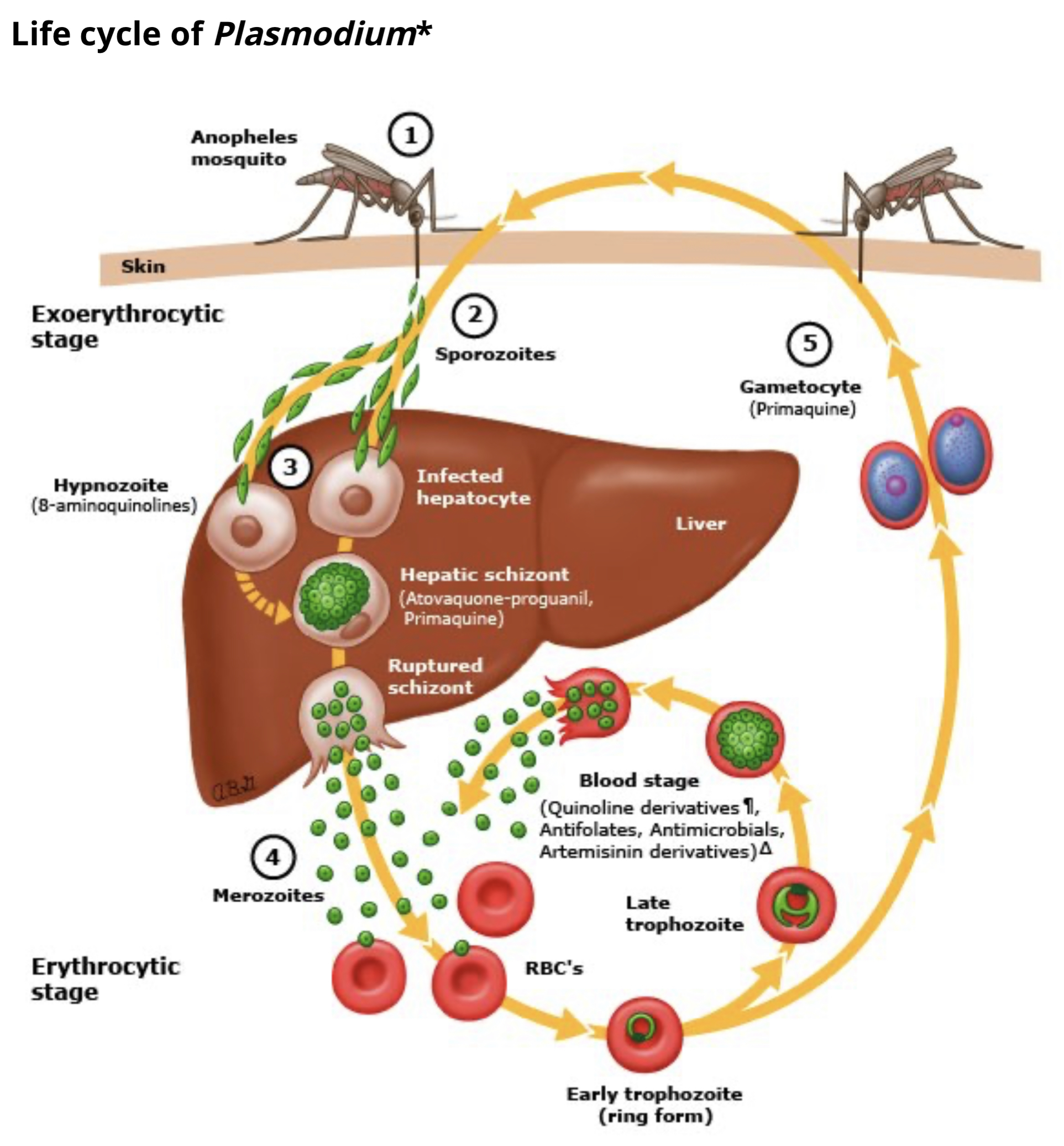
Drug treatment versus parasitic life cycle
![]()
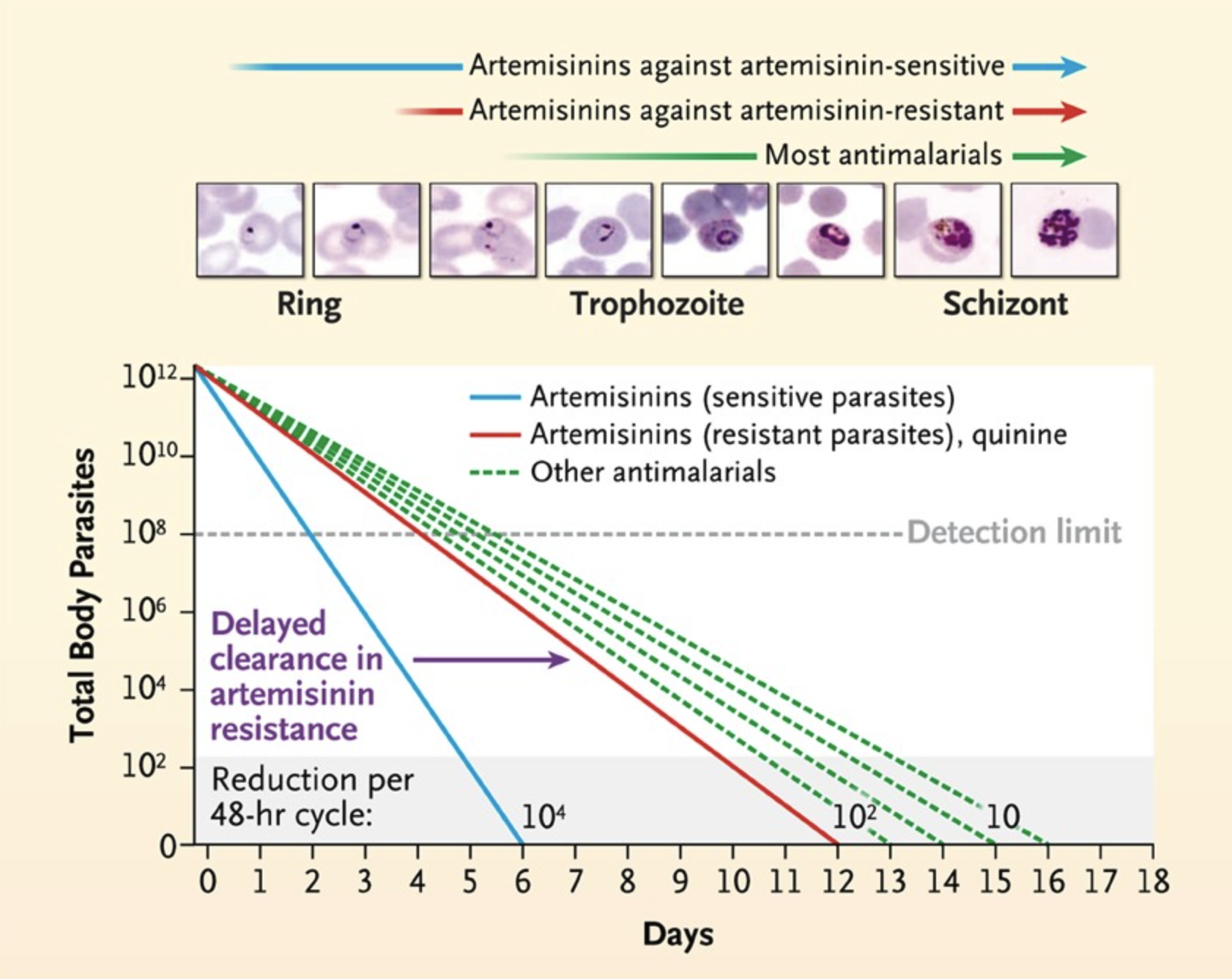
Artemisinin parasite clearance
![]()
Artemisinin-based combination therapy (ACT)
Low side effect profile
Potent against all states (asexual forms) of malaria
Most rapid clearance time relative to other antimalarial drugs
Administered in combination with second drug that has longer half life to forestall artemisinin resistance
WHO recommendations:
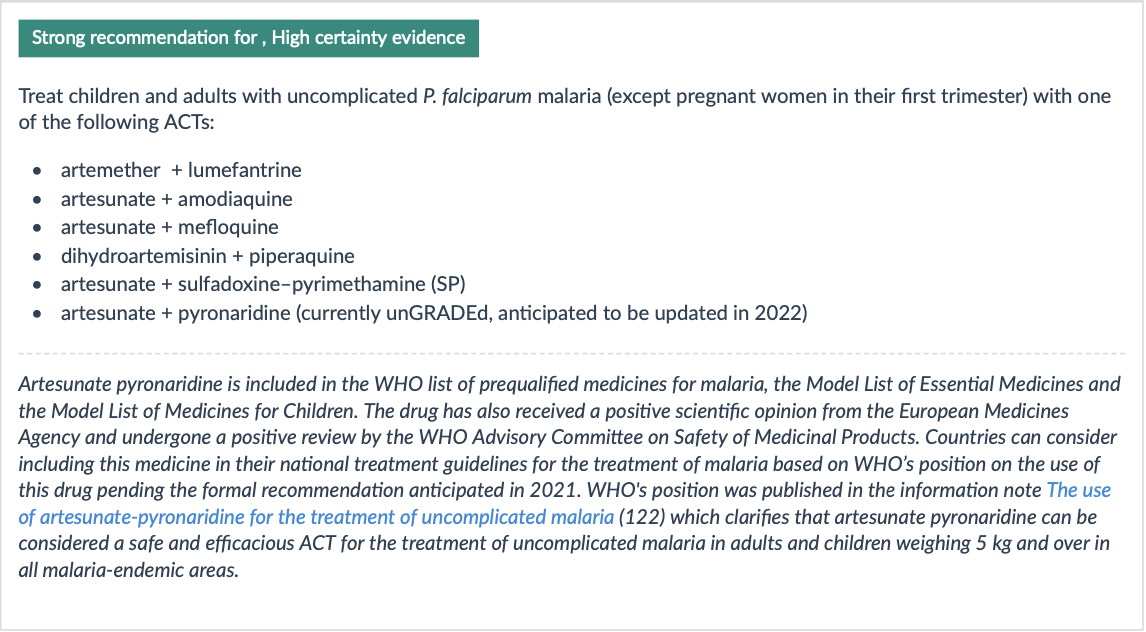
Uncomplicated malaria treatment
![]()
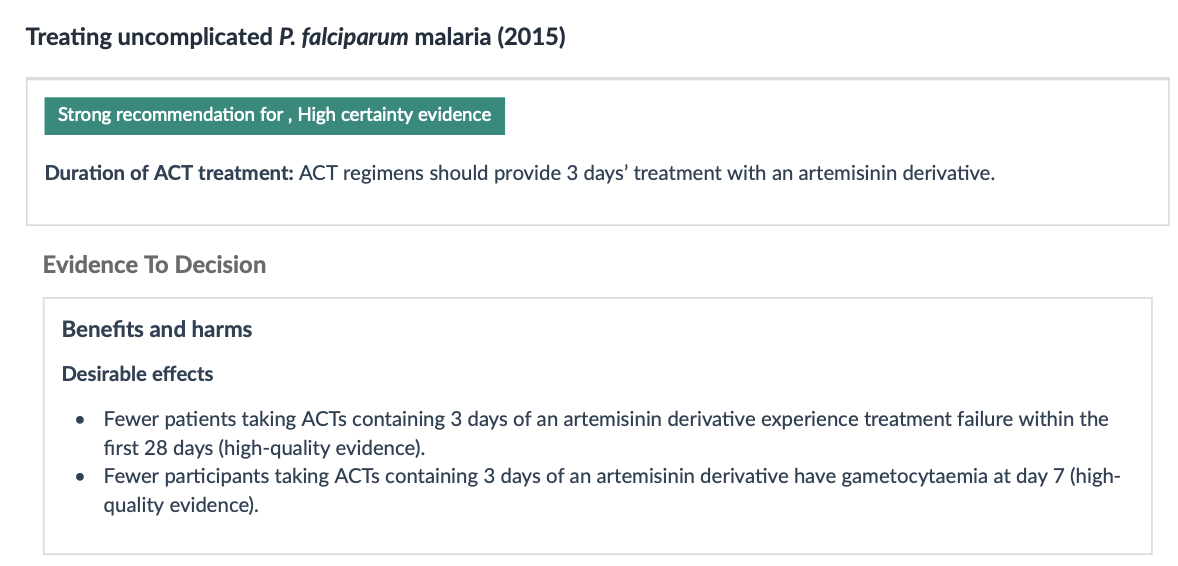
Duration of treatment
![]()
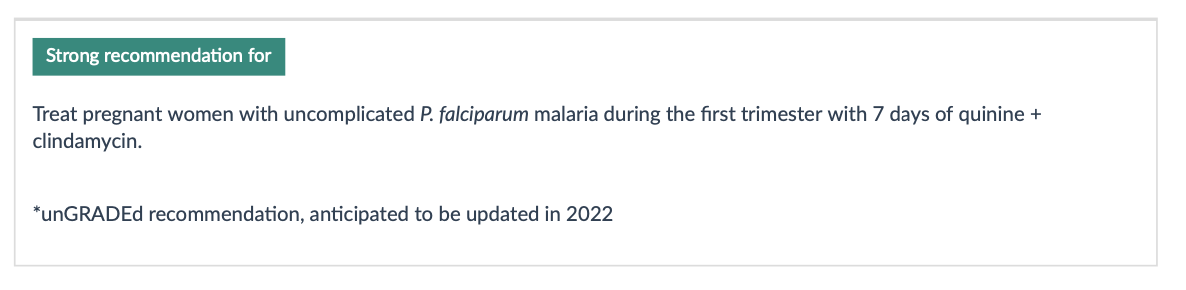
Treatment of pregnant patients
![]()
Relapse or Recurrence
Follow-up blood smears should document clearance of parasitemia within 48-72 hours of appropriate therapy. Follow-up smears every 12-24 hours are common.
Recurrence of P. falciparum malaria can result from re-infection or recrudescence (treatment failure)
Failure :< 28 days: Persistent fever, parasitemia → treat with another ACT regimen effective in region. Treatment with same ACT considered if no second line regimens are available
Failure > 28 days: Likely re-infection: Treat with first-line ACT
Treatment failure may result from:
Drug resistance
Inadequate exposure to the drug due to sub-optimal dosing, poor adherence, vomiting, unusual pharmacokinetics in an individual,
Substandard (counterfeited) medicine
Artemisinin resistance
Southeast Asia, parts of sub-Saharan Africa, South America
Consider in patients with epidemiological exposure
Evaluation:
- Malarial blood smear on day 3: Unlikely if parasite density < 3% with initial parasite density of > 100,000 parasites/μL
Reducing transmissibility
![]()
Reducing transmissibility
- Gametocytes may persist in blood after successful treatment of infection; not harmful to patient but serve as a source of ongoing transmission
- Single doses of primaquine > 0.4 mg/kg bw reduced gametocyte carriage at day 8 by around two thirds (moderate- quality evidence).
![]()
Avoid in pregnant patients and infants < 6 months
======= ## Definition of severe malaria
| Impaired consciousness |
Glasgow coma score <11 in adults or Blantyre coma score <3 in children; inability to swallow |
| Prostration |
Generalized weakness so that a person is unable to sit, stand, or walk without assistance |
| Multiple convulsions |
More than two episodes within 24 hours |
| Acidosis |
A base deficit of >8 mEq/L, a plasma bicarbonate level of <15 mmol/L, or venous plasma lactate ≥5 mmol/L. Clinical indicators of acidosis include rapid, deep, labored breathing. |
| Hypoglycaemia |
Blood or plasma glucose <40 mg/dL (<2.2 mmol/L) for children ≥5 years and adults; blood or plasma glucose <54 mg/dL (<3 mmol/L) for children <5 years |
| Severe anaemia |
Haemoglobin concentration ≤5 g/dL or hematocrit ≤15% in children <12 years of age (<7 g/dL and <20%, respectively, in adults) with parasite count >10,000 parasites/uL |
| Renal impairment |
Plasma or serum creatinine >3 mg/dL (265 umol/L) or blood urea >20 mmol/L |
| Jaundice |
Plasma or serum bilirubin >50 umol/L (3 mg/dL) with one of the following:
- Plasmodium falciparum parasite count >2.5% parasitemia
- Plasmodium knowlesi parasite count >20,000 parasites/uL |
| |
Pulmonary edema | Radiographically confirmed or oxygen saturation <92% on room air with respiratory rate >30/minute, often with chest indrawing and crepitation on auscultation |
======= | Pulmonary edaema | Radiographically confirmed or oxygen saturation <92% on room air with respiratory rate >30/minute, often with chest indrawing and crepitation on auscultation | | Significant bleeding | Including recurrent or prolonged bleeding (from the nose, gums, or venipuncture sites), hematemesis, or melena | | Shock | Compensated shock is defined as capillary refill ≥3 seconds or temperature gradient on leg (mid to proximal limb), but no hypotension. Decompensated shock is defined as systolic blood pressure <70 mmHg in children or <80 mmHg in adults, with evidence of impaired perfusion (cool peripheries or prolonged capillary refill). | | Hyperparasitaemia | P. falciparum:
- In non-immune travelers: parasitemia ≥5%[3]
- All patients: parasitemia >10%
P. knowlesi:
- Parasite density >100,000 parasites/uL
Plasmodium vivax:
- No established parasite density thresholds |
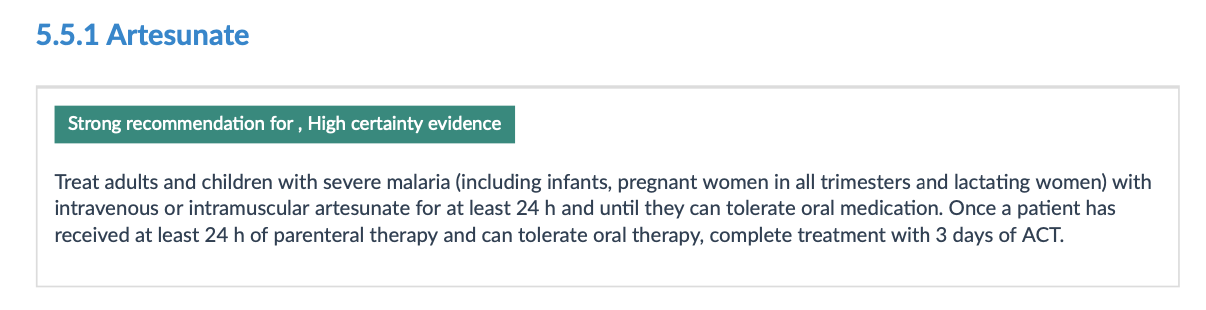
Treatment of severe malaria
![]()
Delayed haemolysis starting >1 week after artesunate treatment of severe malaria has been reported in hyperparasitaemic non-immune travellers.
When artesunate not available, artemether is considered as second line therapy followed by quinine (dihyrdochloride)- must be given by slow infusion or IM.
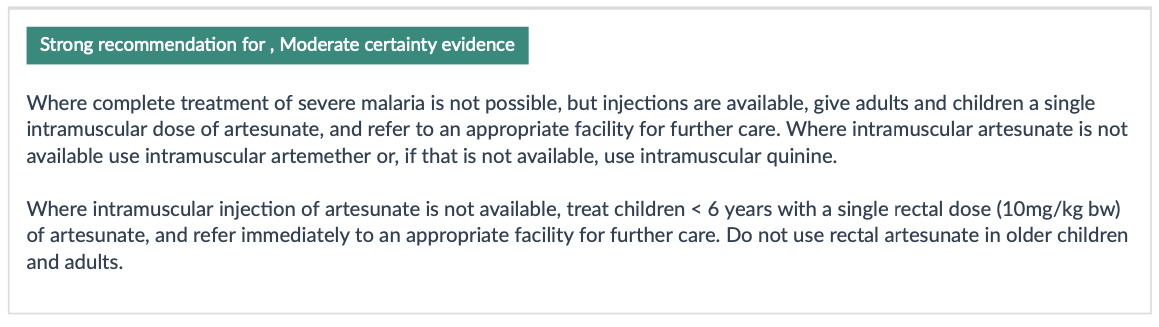
Pre-referral treatment options
![]()
Prevention of malaria infection in travellers
Vaccine prospects
![]()
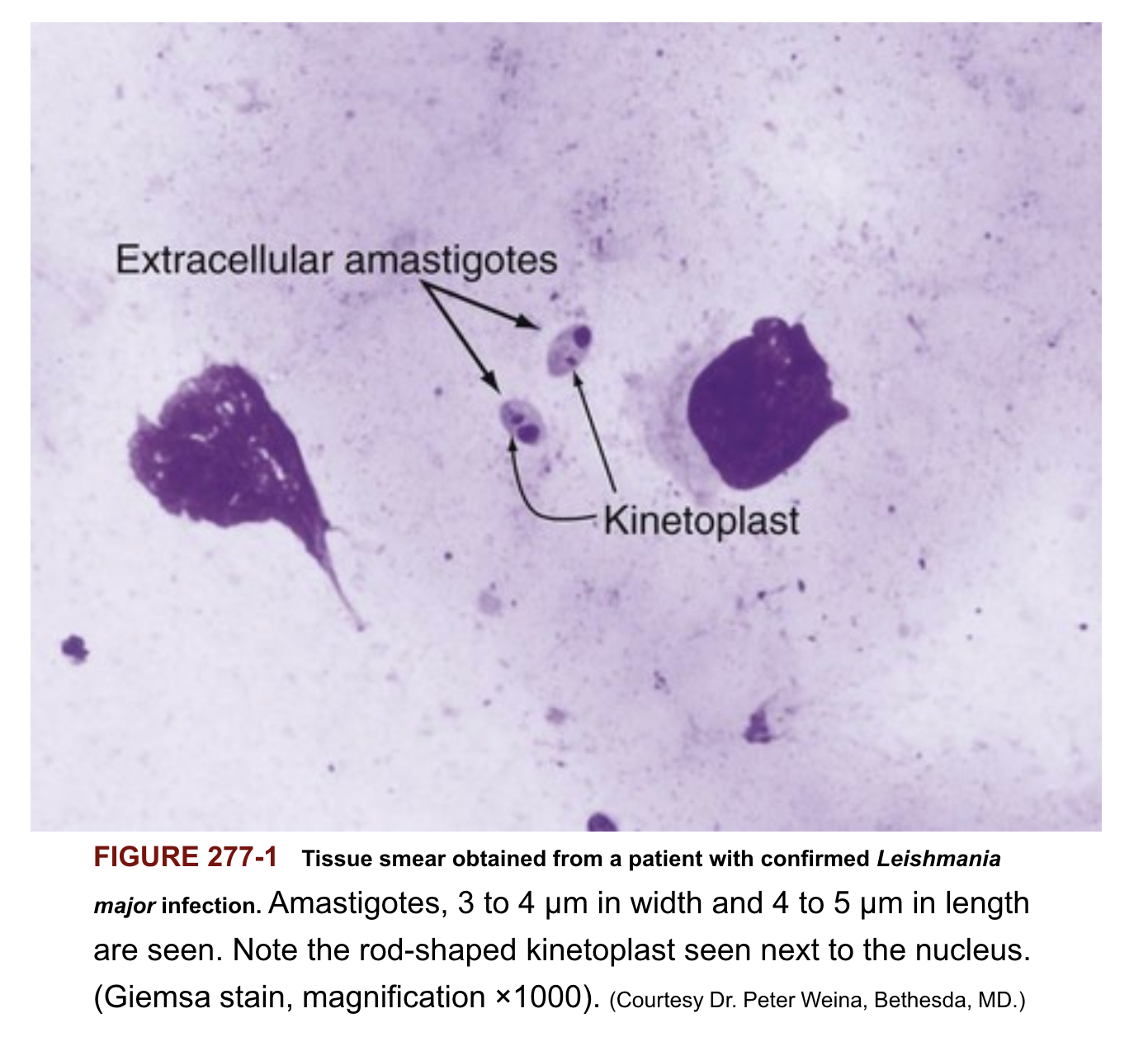
Tissue smear from patient with Leishmania
![]()
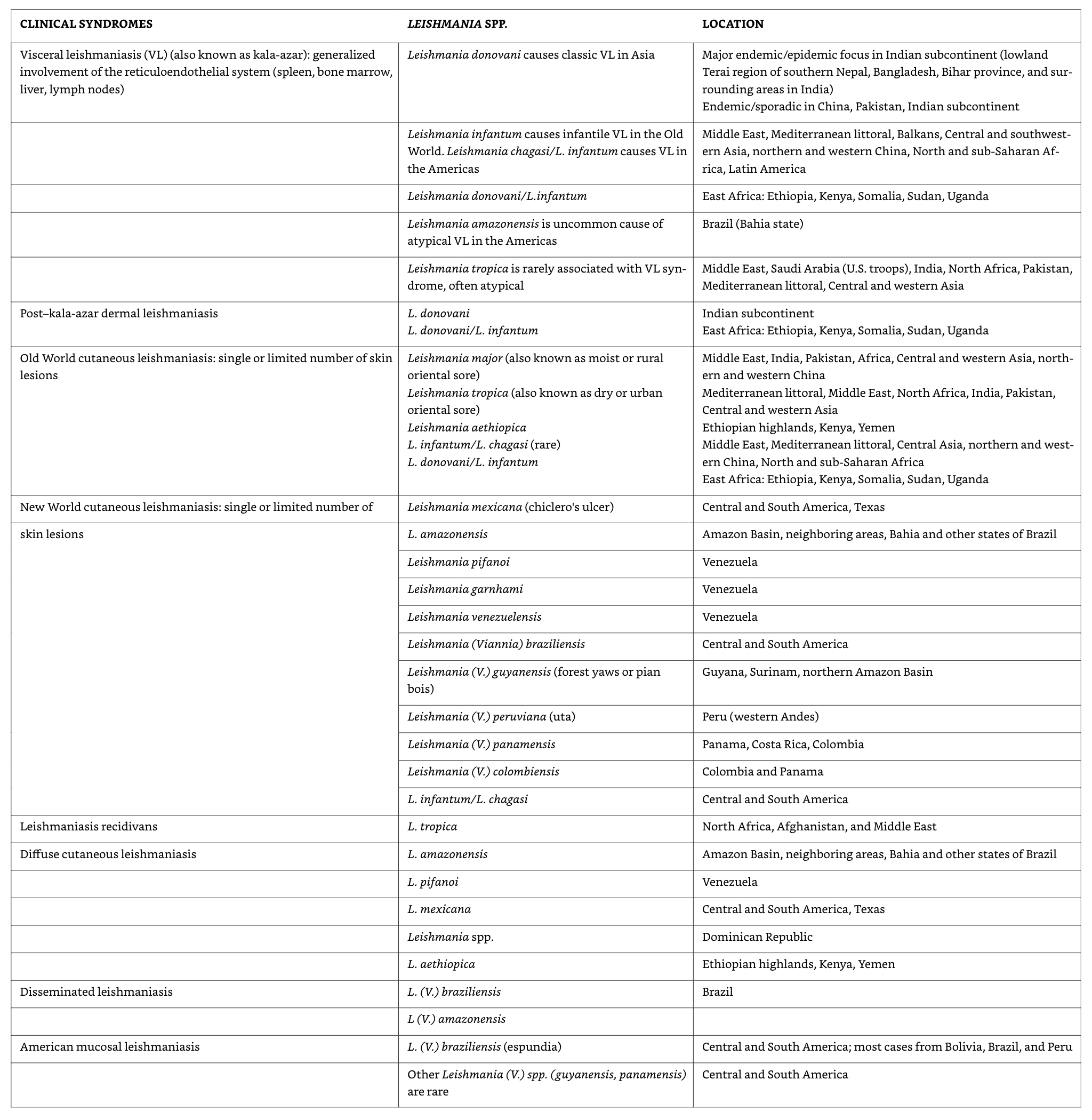
Leishmaniasis classification
![]()
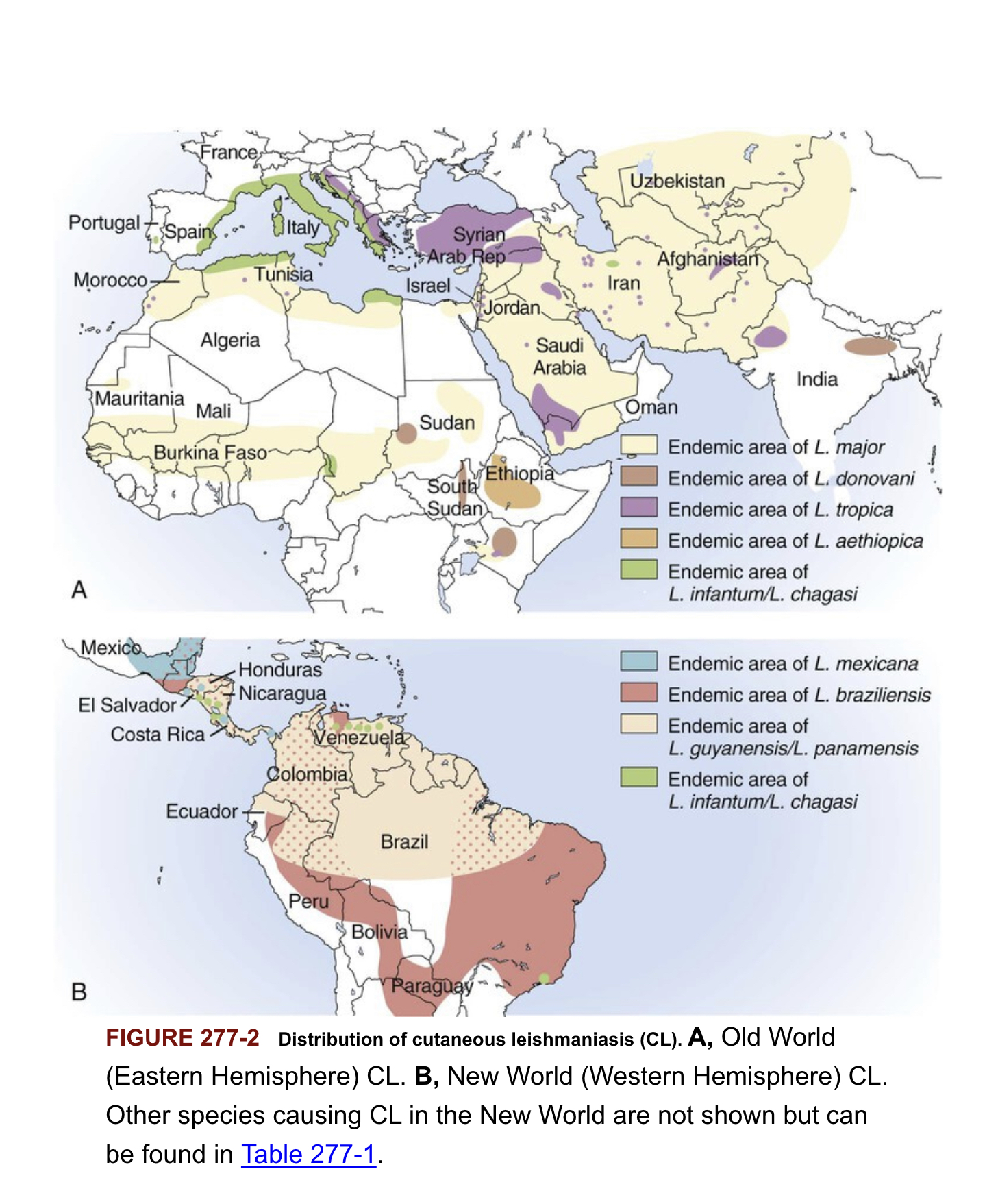
Distribution of cutaneous leishmaniasis
![]()
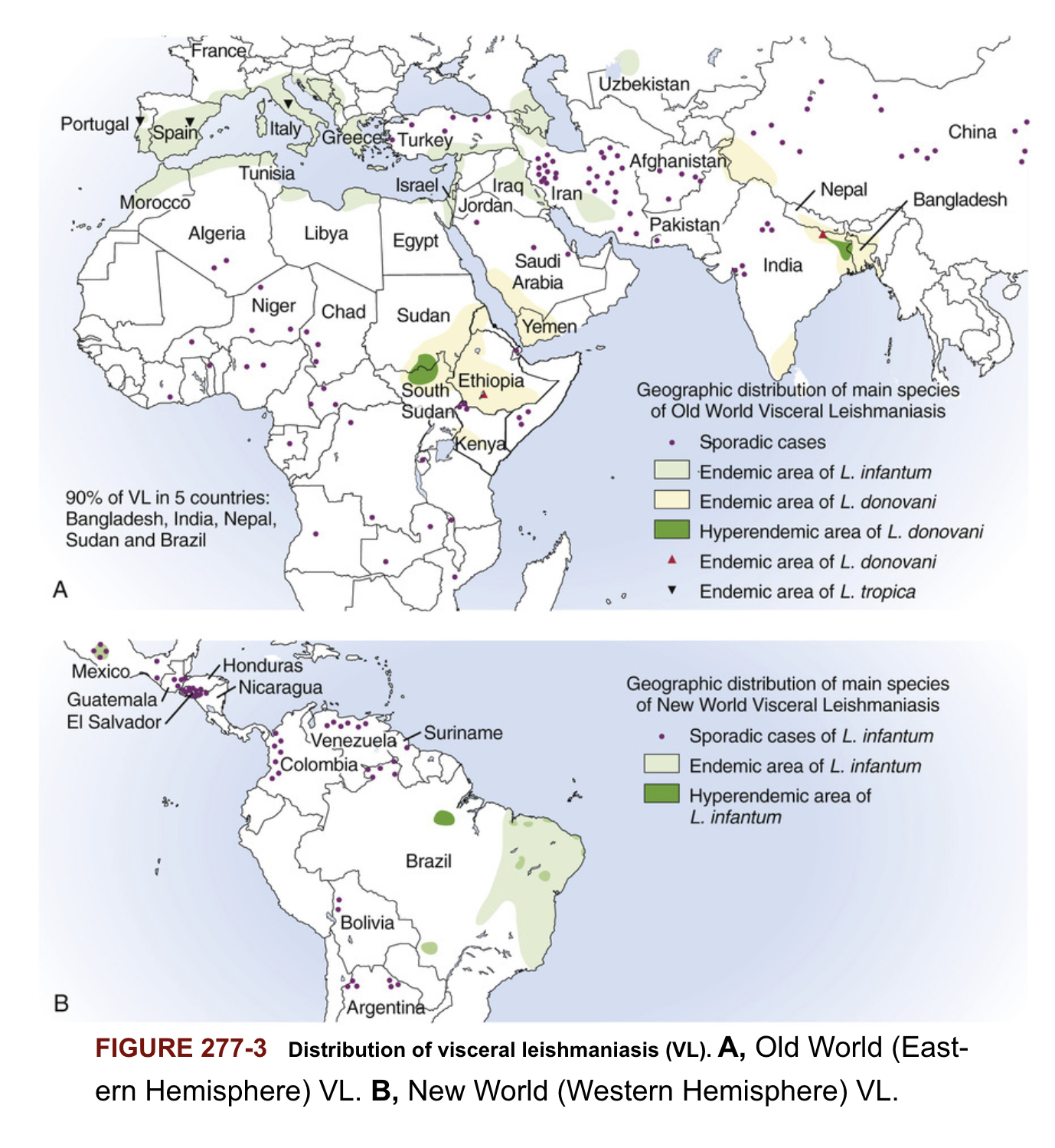
Distribution of visceral leishmaniasis
![]()
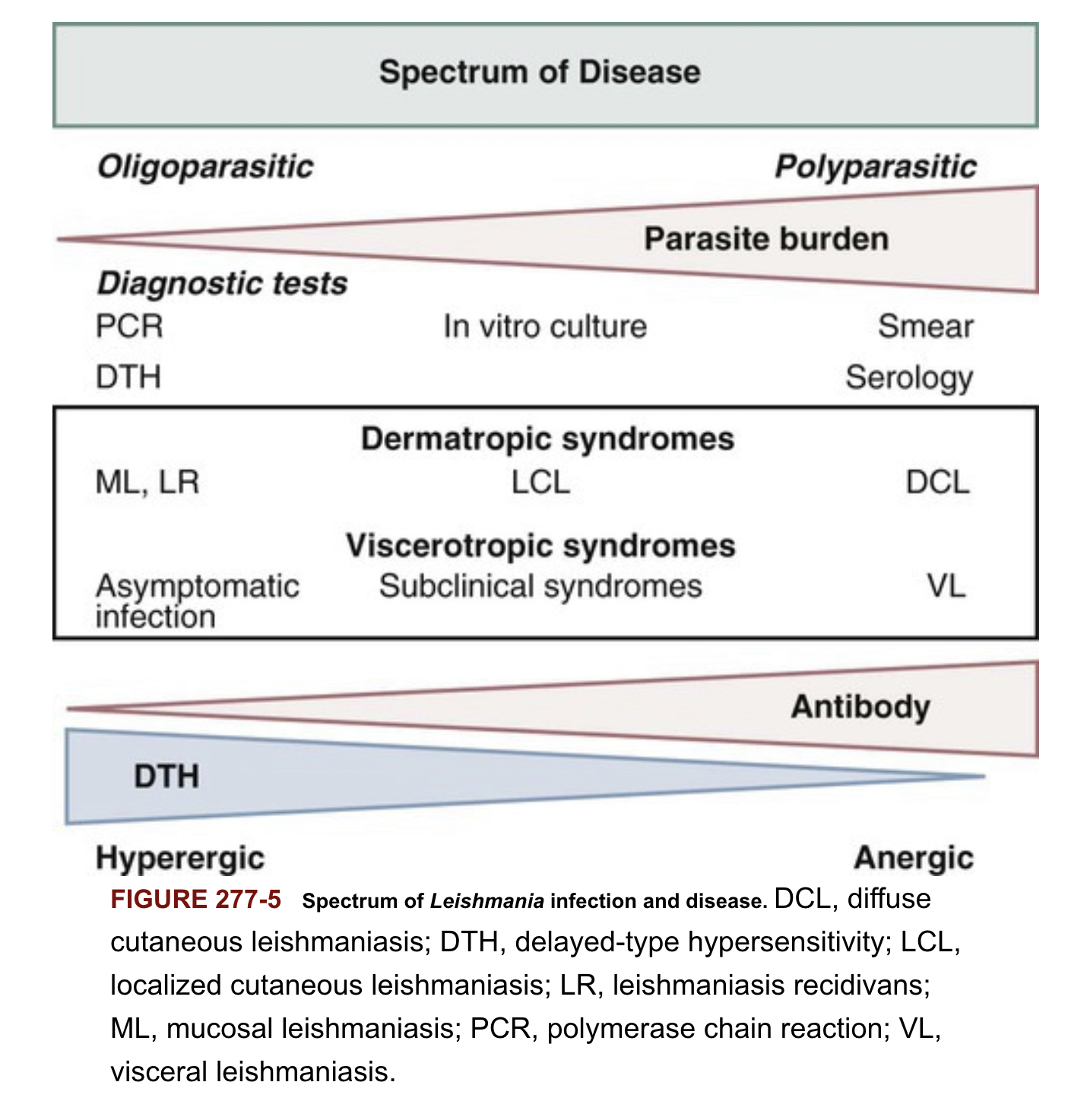
Spectrum of Leishmania infection and disease
![]()
Pathophysiology
Leishmania invade and replciate inside host macrophages
Many infections are asymptomatic (subclinical), reflecting the host ability to control the infection
Subclinical infections can reactive during periods of immunosuppression
Classic presentation of VL (kala-azar)
- Prolonged fever
- Weight loss
- Hepato- splenomegaly
- Parasite replicate in reticuloendothelial system (RES), with high parasite loads accumulating in liver, spleen and bone marrow
- Pancytopenia (due to bone marrow suppression)
- Hypergammaglobinumia (polyclonal B cell activation)
- Late in course of infection thrombocytopenia and liver dysfunction
- Uniformly lethal without treatment
Clinical manifestations
- incubation period (2-8 months) but can be as short as 8 10 days
- Clinical disease may first become symptomatic years after exposure in patients who are immunocompromised
- Insidious development: fever, weakness, loss of appetite, weightloss, failure to thrive, abdominal enlargement caused by hepatosplenomegaly
- Acute presentation in non-immune patients with high fever and chills, sometimes with a periodicity suggestive of malaria
- Spleen can become massively enlarges, soft and non-tender -Elevated liver enzymes and bilirubin occasionally present
- Patients often become cachectic with petechia and ecchymoses with possible epistaxis and gingival bleeding
Protruding abdomen with hepatosplenomegaly
![]()
Diagnosis Pentad
- Prolonged fever
- Progressive weight-loss
- Pronounced spelnomegaly
- Pancytopenia
- Hypergammaglobulinemia
Diagnosis confirmation
- Parasitologic diagnosis: Amastigotes in tissues
- Isolation of promastigotes in cultures
- Splenic aspiration, liver biopsy, lymph node or bone marrow aspirates (safer but lower sensitivity)
- PCR assay
- Antileishmanial antibodies
Treatment
- Liposomal amphotericin B 10 mg/kg two consecutive days or 3 mg/kg days 1-5, 14, and 21
- Amphotericin B deoxycholate 1 mg/kg for 15 days or 1 mg/kg every other day for 30 days
- Pentamidine (hypotension, hypoglycaemia, insulin-dependent diabetes mellitus)
- Miltefosine (oral, GI toxicity, elevated liver transaminases)
Treatment response
- Fever resolution (1-2 weeks)
- Decrease in spleen size over 1 month
- Weight gain
- Patients need to be followed for 12 month and instructed to return if symptoms recur.
Dondorp AM, Fairhurst RM, Slutsker L, MacArthur JR, M. D. JGB, Guerin PJ, et al. The threat of artemisinin-resistant malaria. New England Journal of Medicine 2011;365:1073–5.
https://doi.org/10.1056/NEJMp1108322.
Fairhurst, Rick, Wellems, Thomas. Malaria (plasmodium species). 8th ed., Elsivier; 2015.
Idro R, Jenkins NE, Newton CR. Pathogenesis, clinical features, and neurological outcome of cerebral malaria. The Lancet Neurology 2005;4:827–40.
https://doi.org/10.1016/S1474-4422(05)70247-7.
Organization WH. WHO Guidelines for Malaria 2022.
Phillips MA, Burrows JN, Manyando C, Huijsduijnen RH van, Van Voorhis WC, Wells TNC. Malaria. Nature Reviews Disease Primers 2017;3:17050.
https://doi.org/10.1038/nrdp.2017.50.
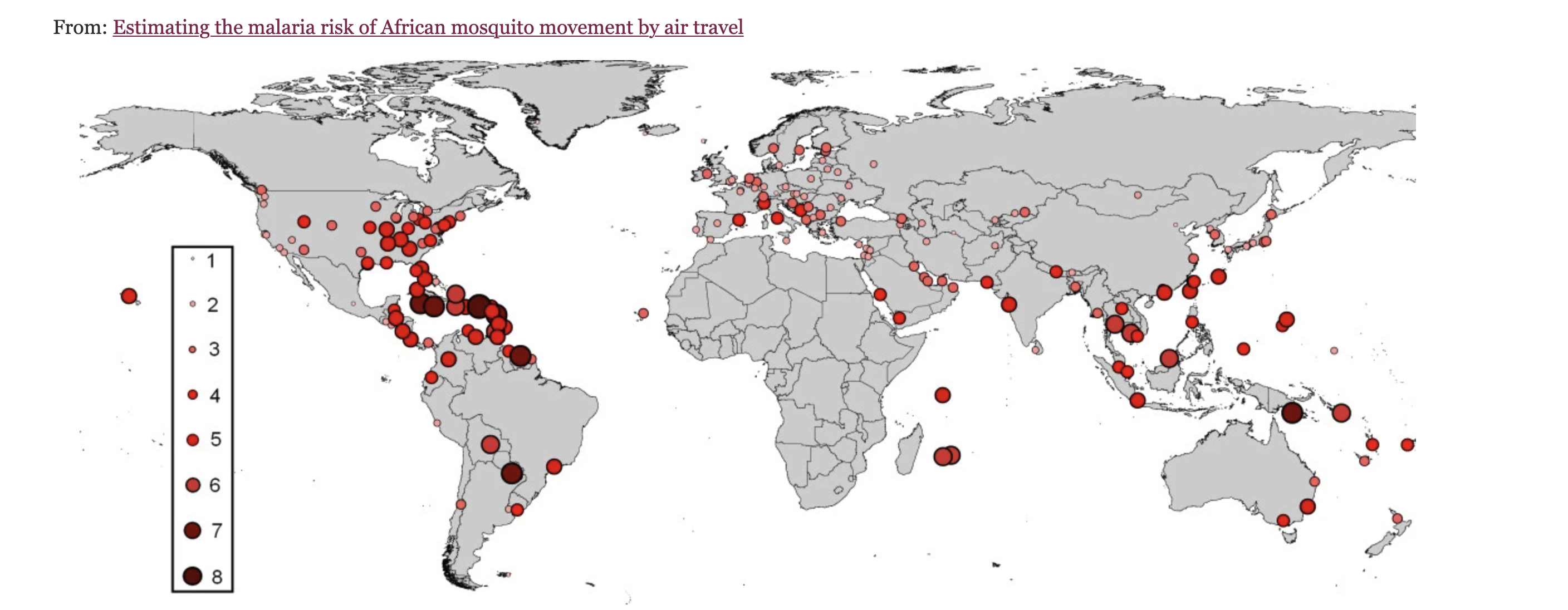
Tatem AJ, Rogers DJ, Hay SI. Estimating the malaria risk of african mosquito movement by air travel. Malaria Journal 2006;5:57.
https://doi.org/10.1186/1475-2875-5-57.