Fever of Unknown Origin (FUO)
Fever of unknown origin (FUO)
Russell Lewis
Associate Professor, Infectious Diseases
Department of Molecular Medicine
MEP 2491 Infectious Diseases
13 March 2023

Febris- Roman Goddess of Fever

The legend of Febris was said to center around the haunting marshes of Camagna in Southern Italy where like clockwork every year, the people would become deathly ill with a mysterious disease. She was so feared by the Romans that the suffering population had created a cult to Febris. They went so far as to wear protective amulets and build her temples in order to worship her to win her favour.
Galileo and the room thermometer in Padova
Fever in modern medicine
Wunderlich’s pioneering studies of thermometry-normal 37°C
Since the 19th century, humans have become gradually colder-0.05° to 0.5°C per decade
Current normal range is 36.3 to 36.5°C
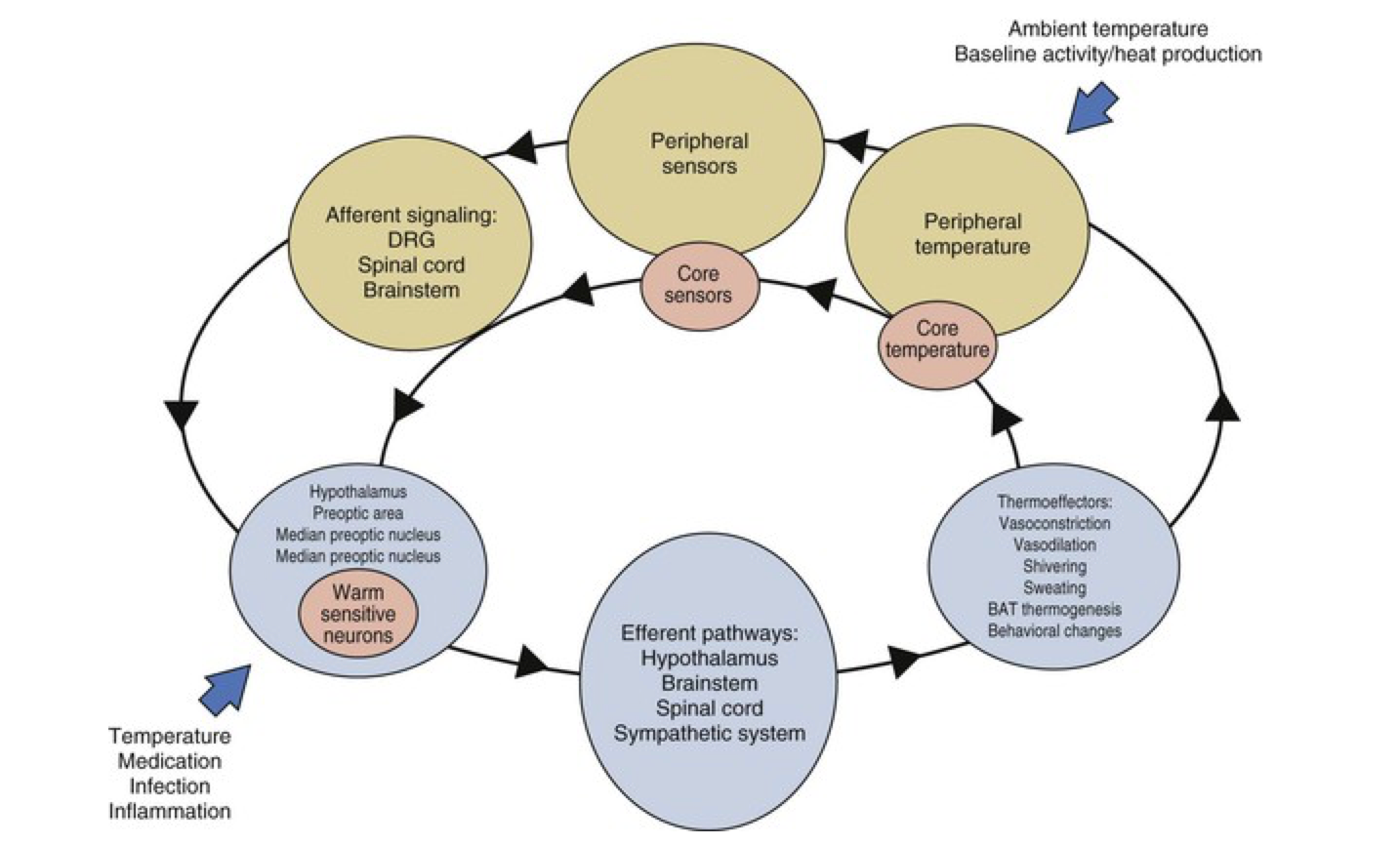
Thermal homeostasis
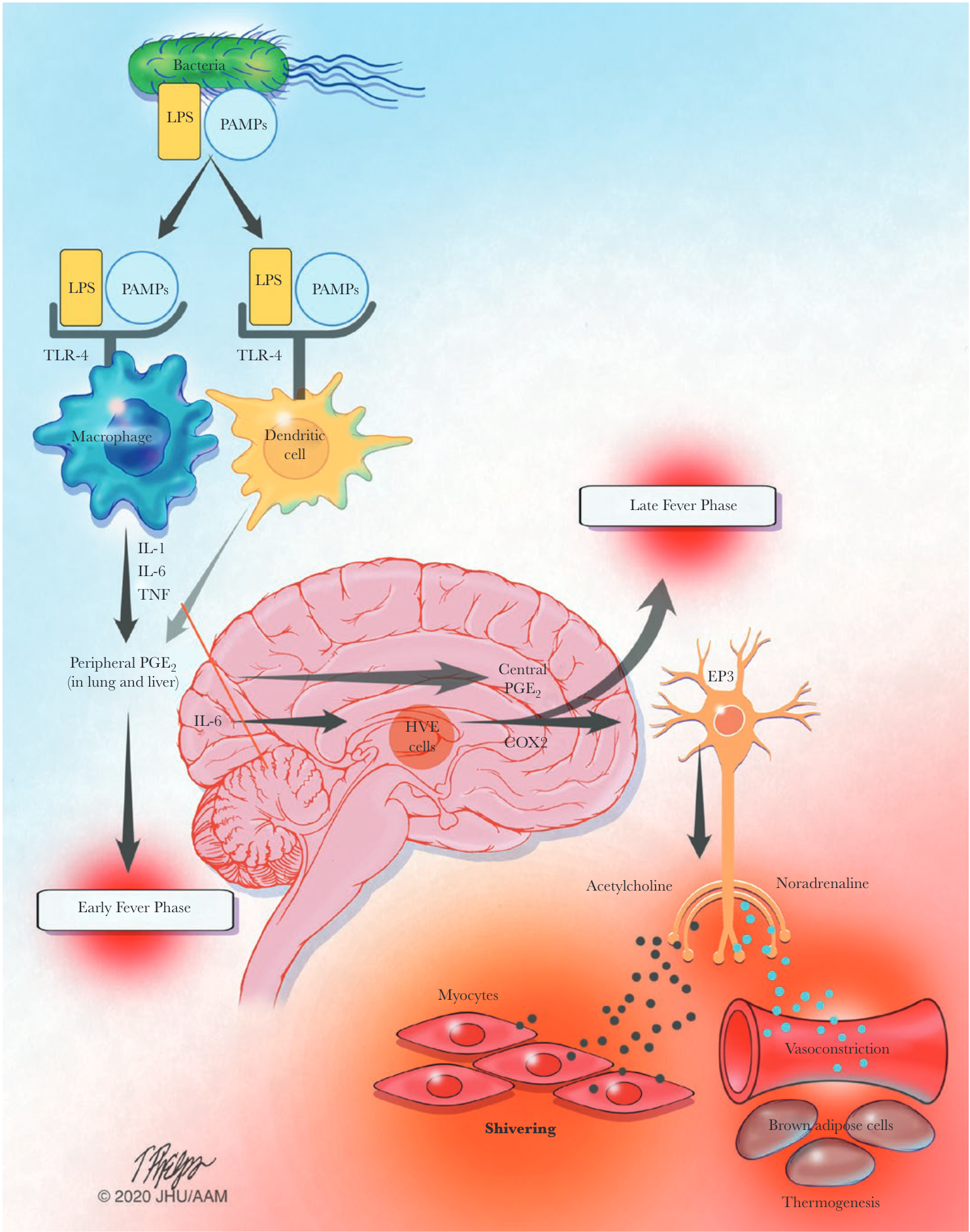
Infection-associated fever
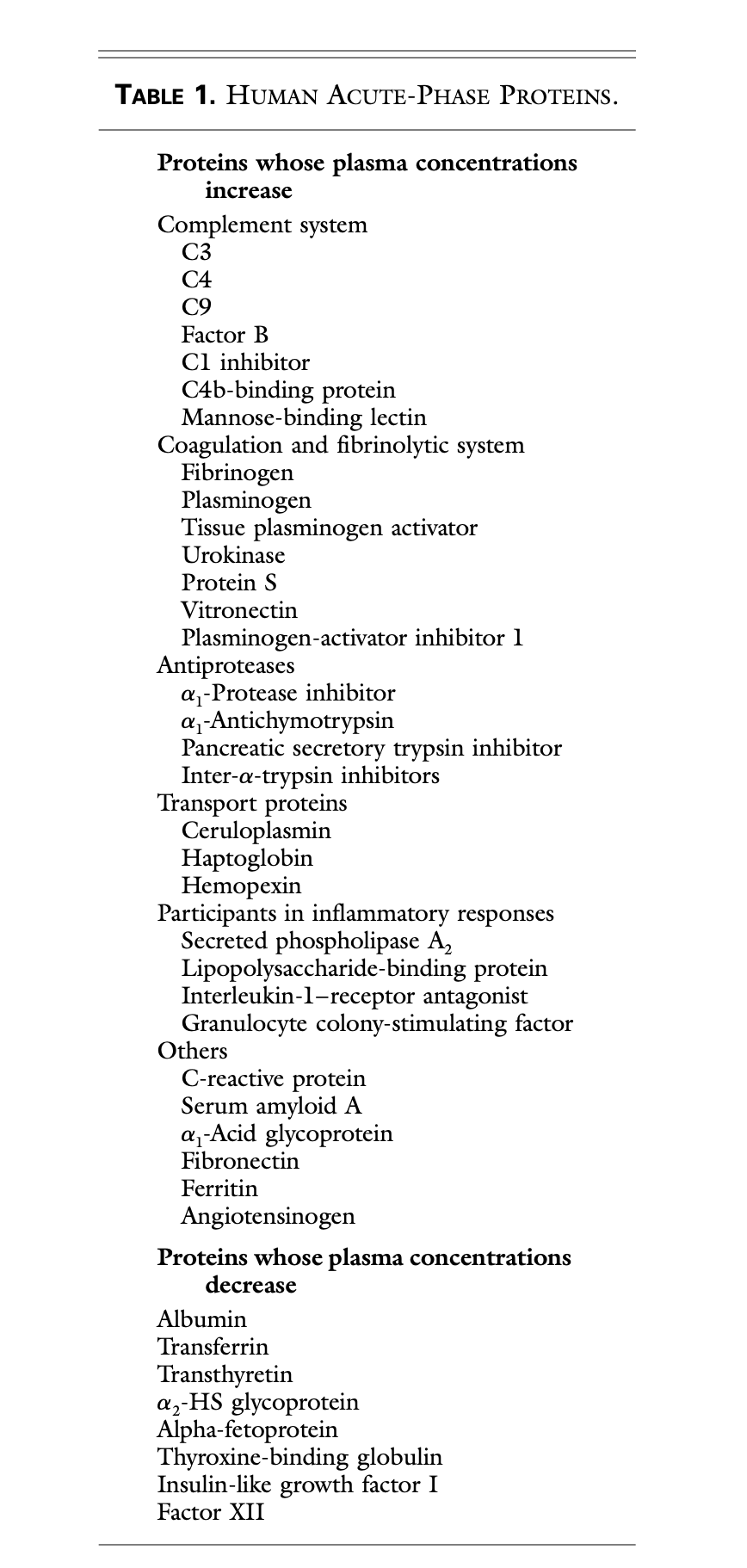
Acute phase proteins
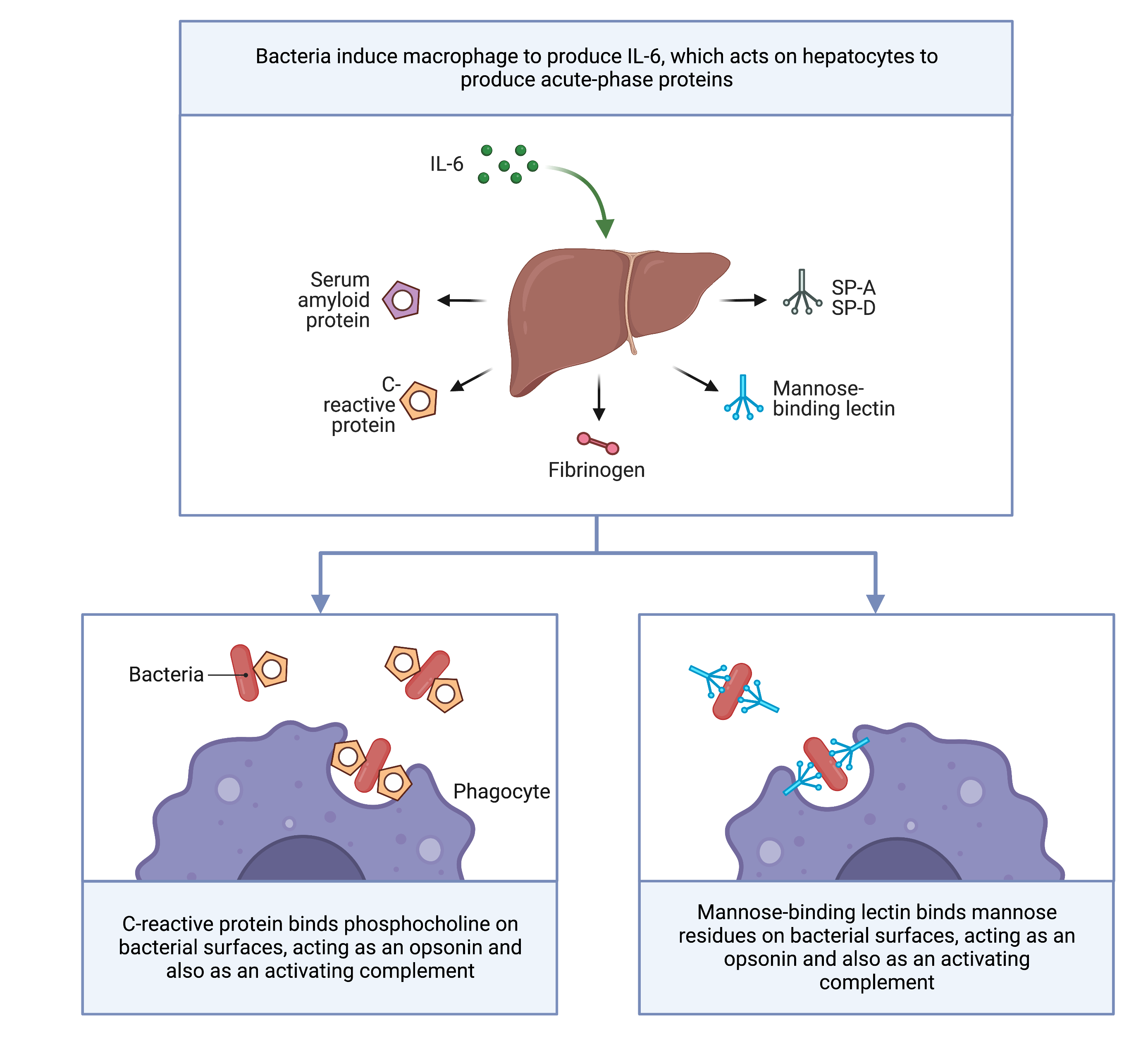
Role of acute phase proteins
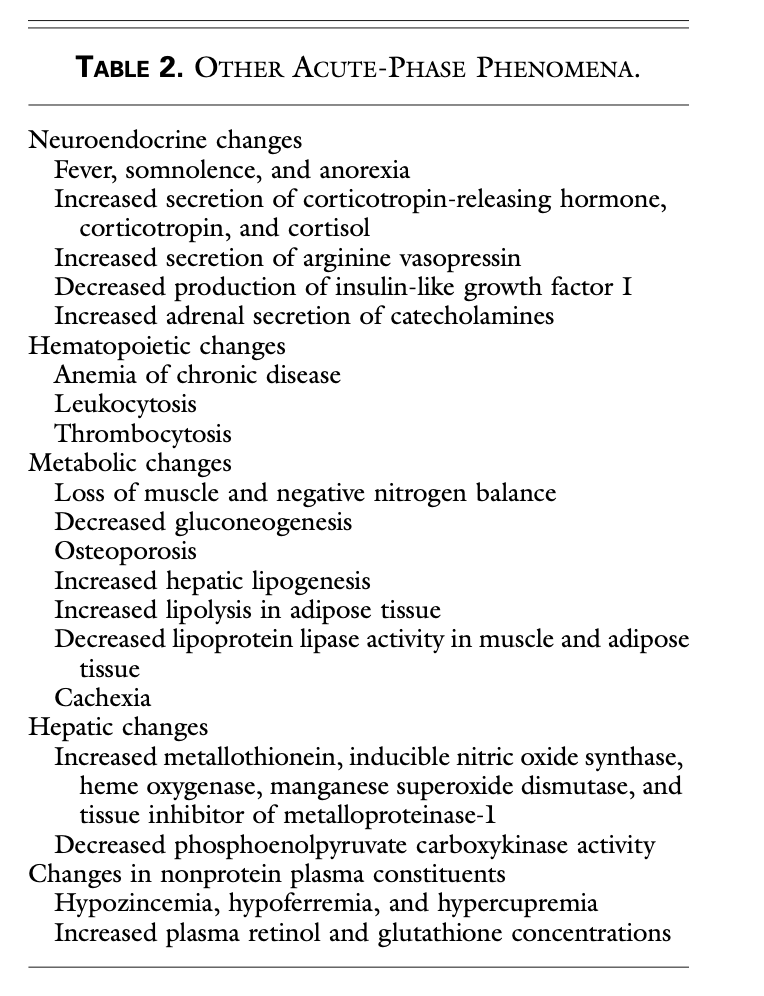
Acute phase phenomena
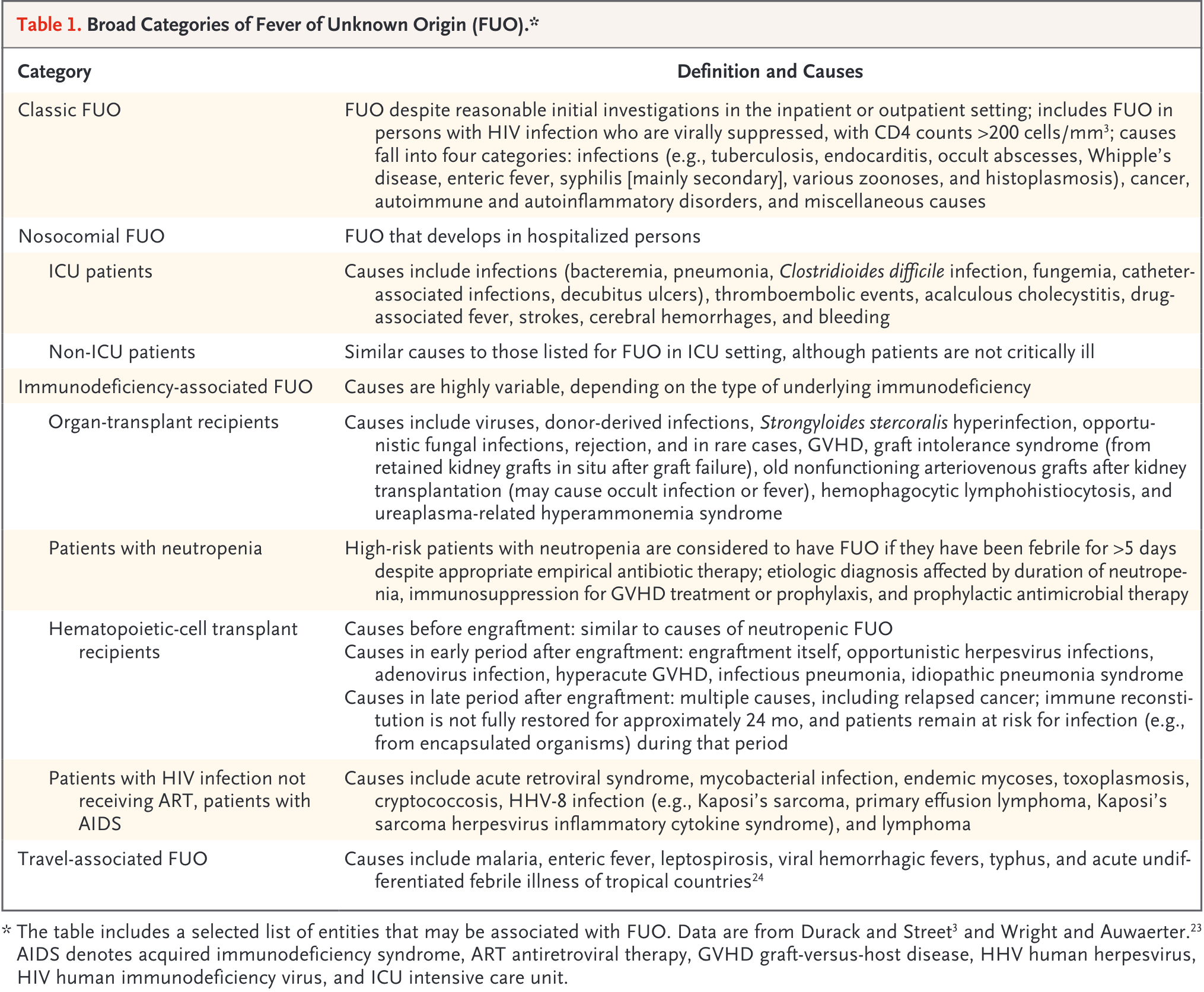
Epidemiology of FUO- Definitions
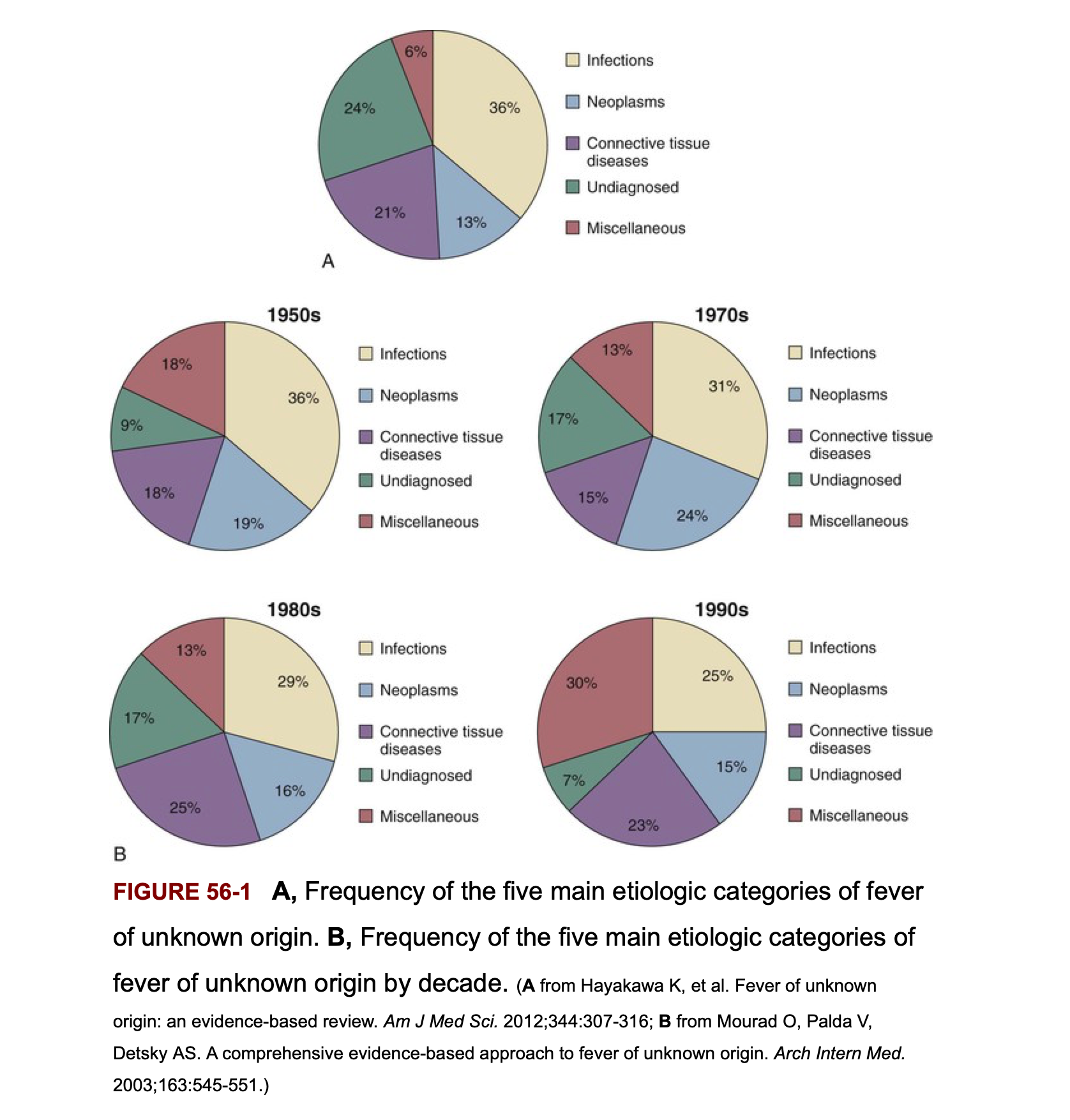
Frequency of the 5 main etiologic categories of FUO
Infectious causes decrease in patients above age 65 years
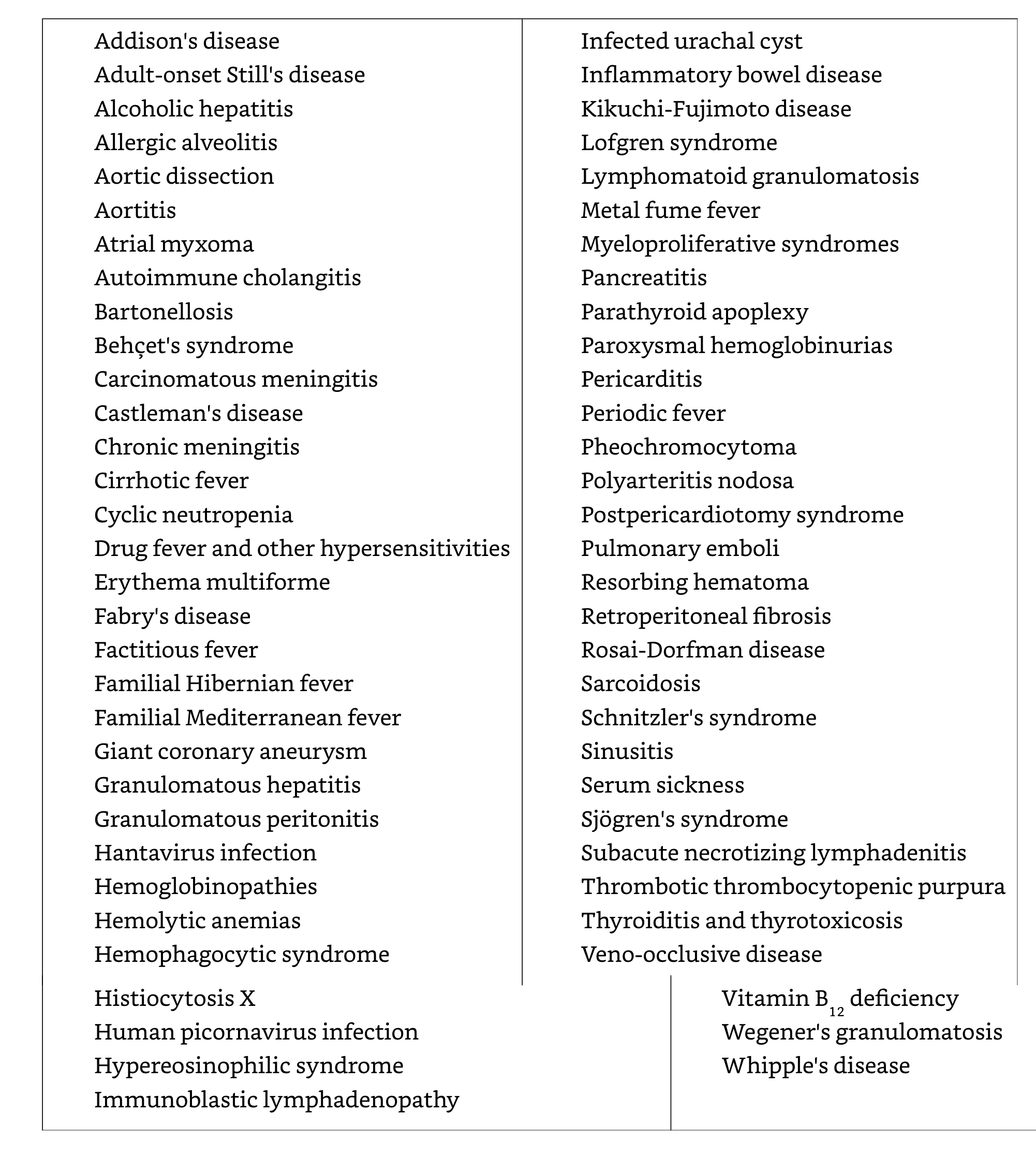
Rare and miscellaneous causes of fever
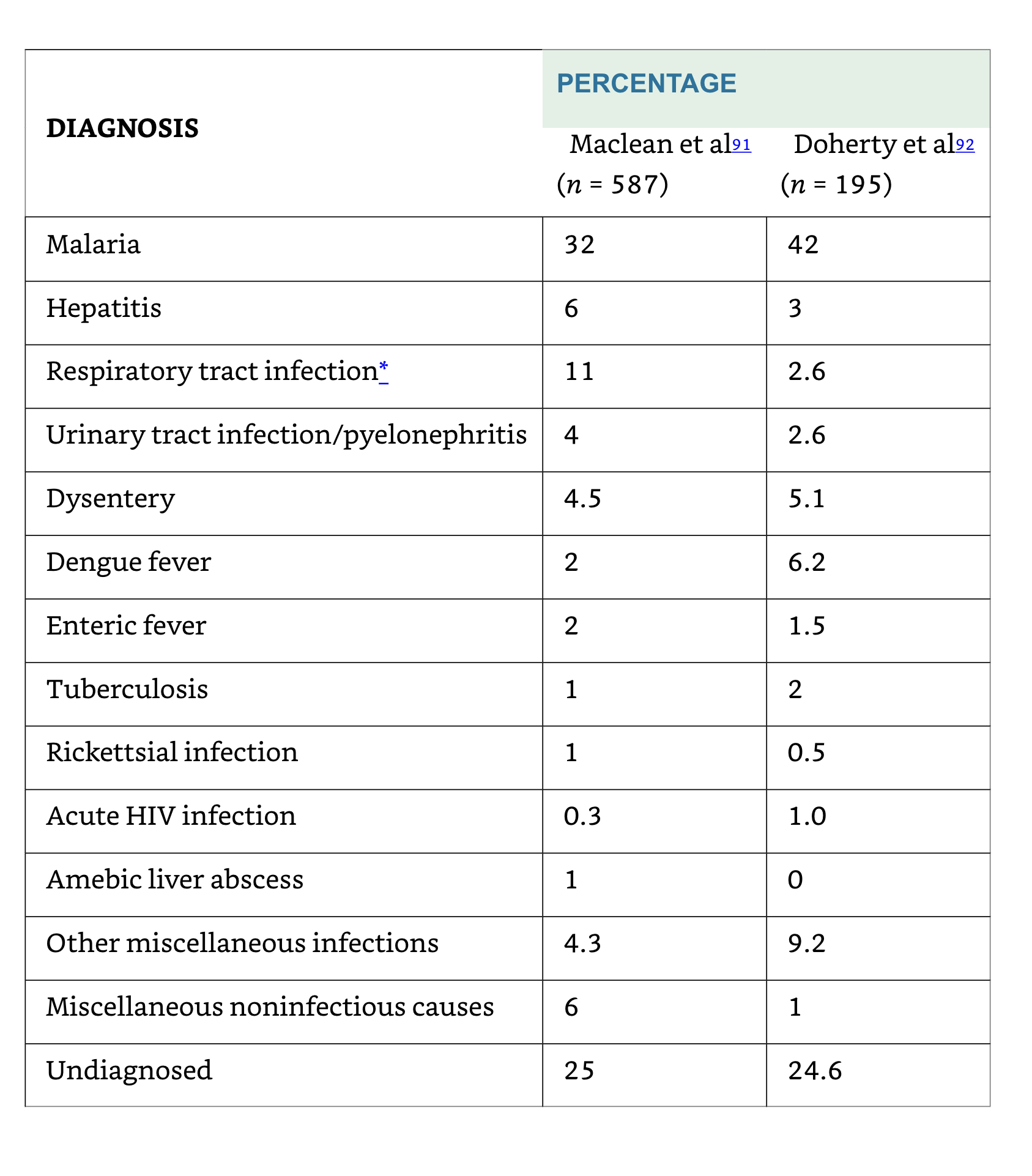
Returning travellers
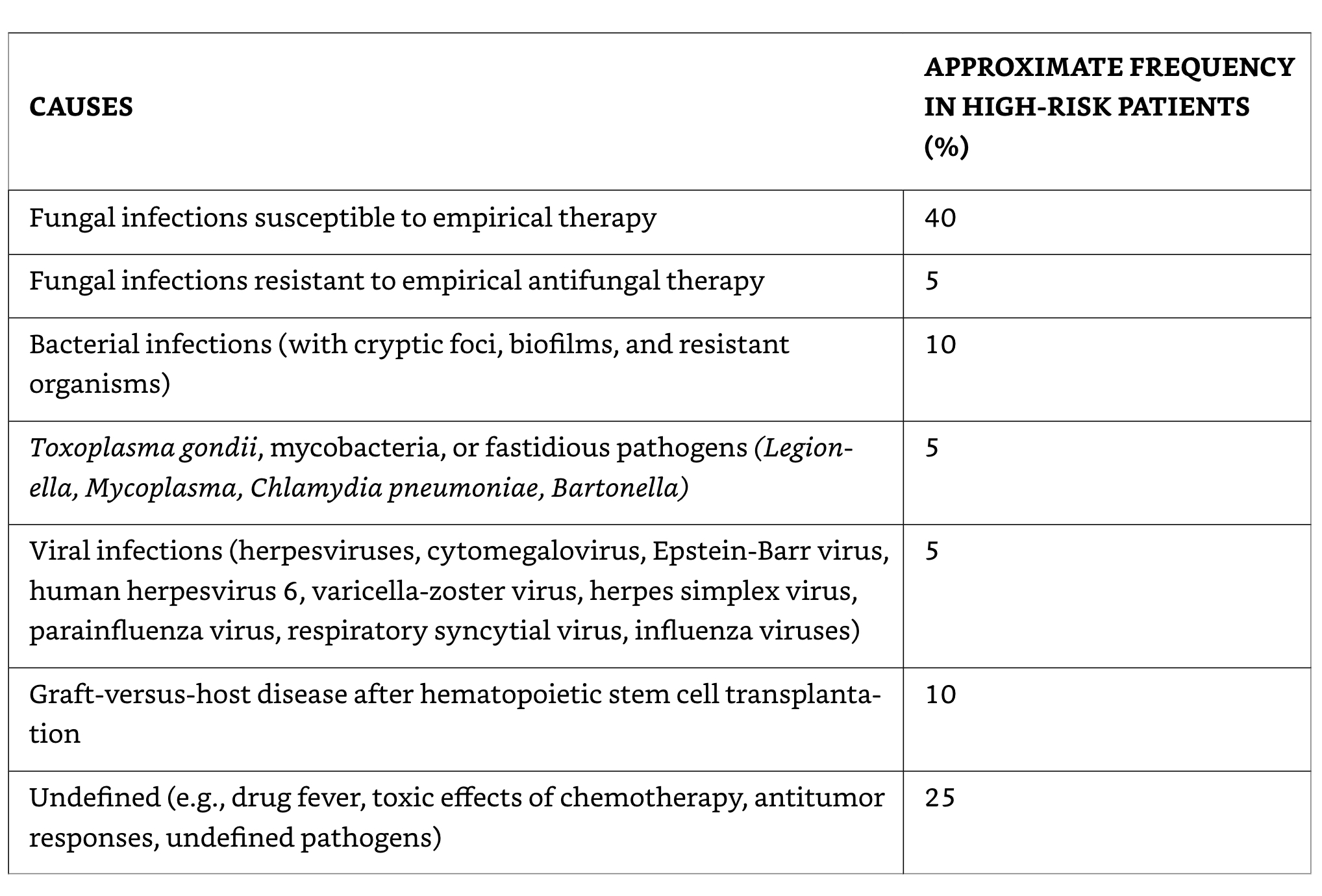
Possible causes of fever in neutropenic patients not responding to broad-spectrum antibiotics
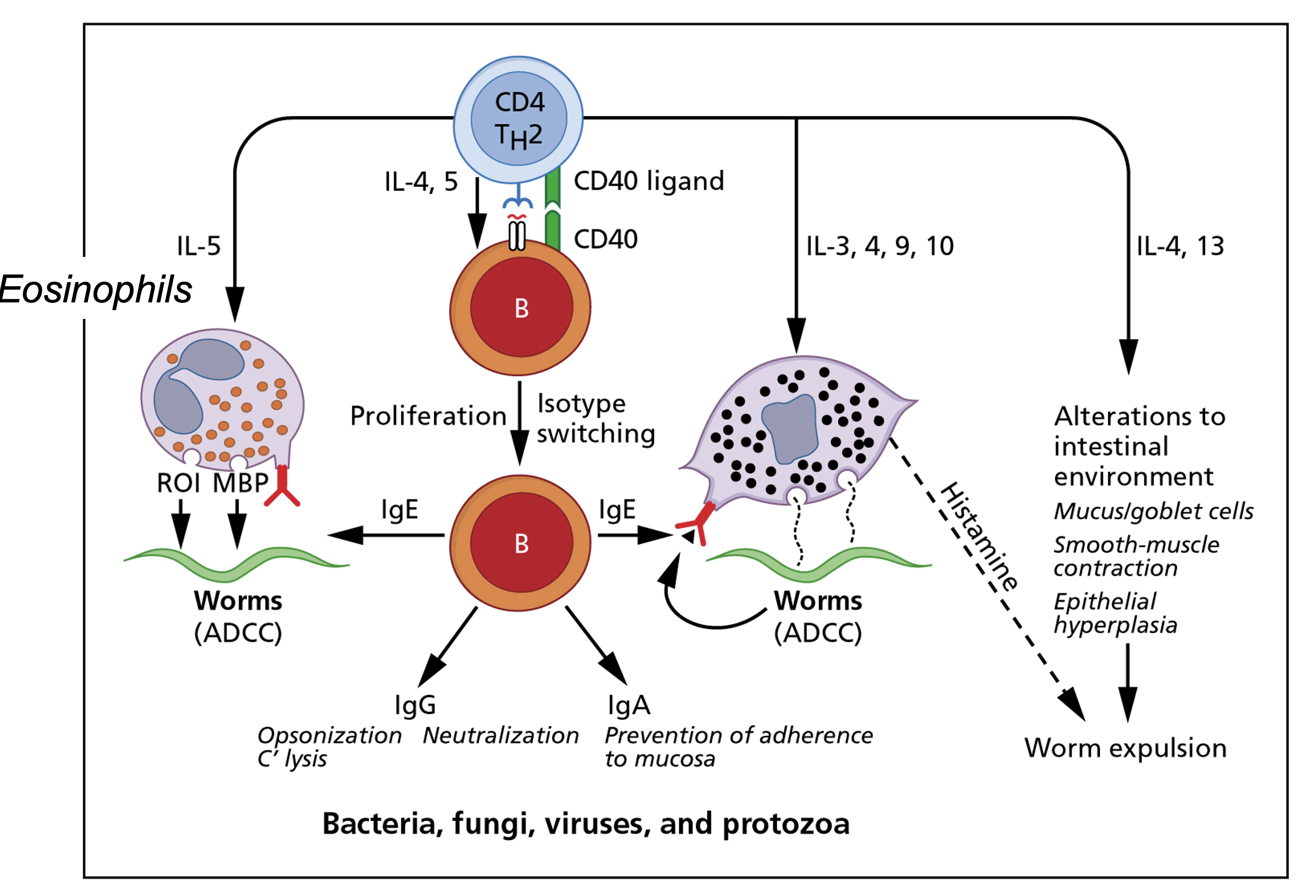
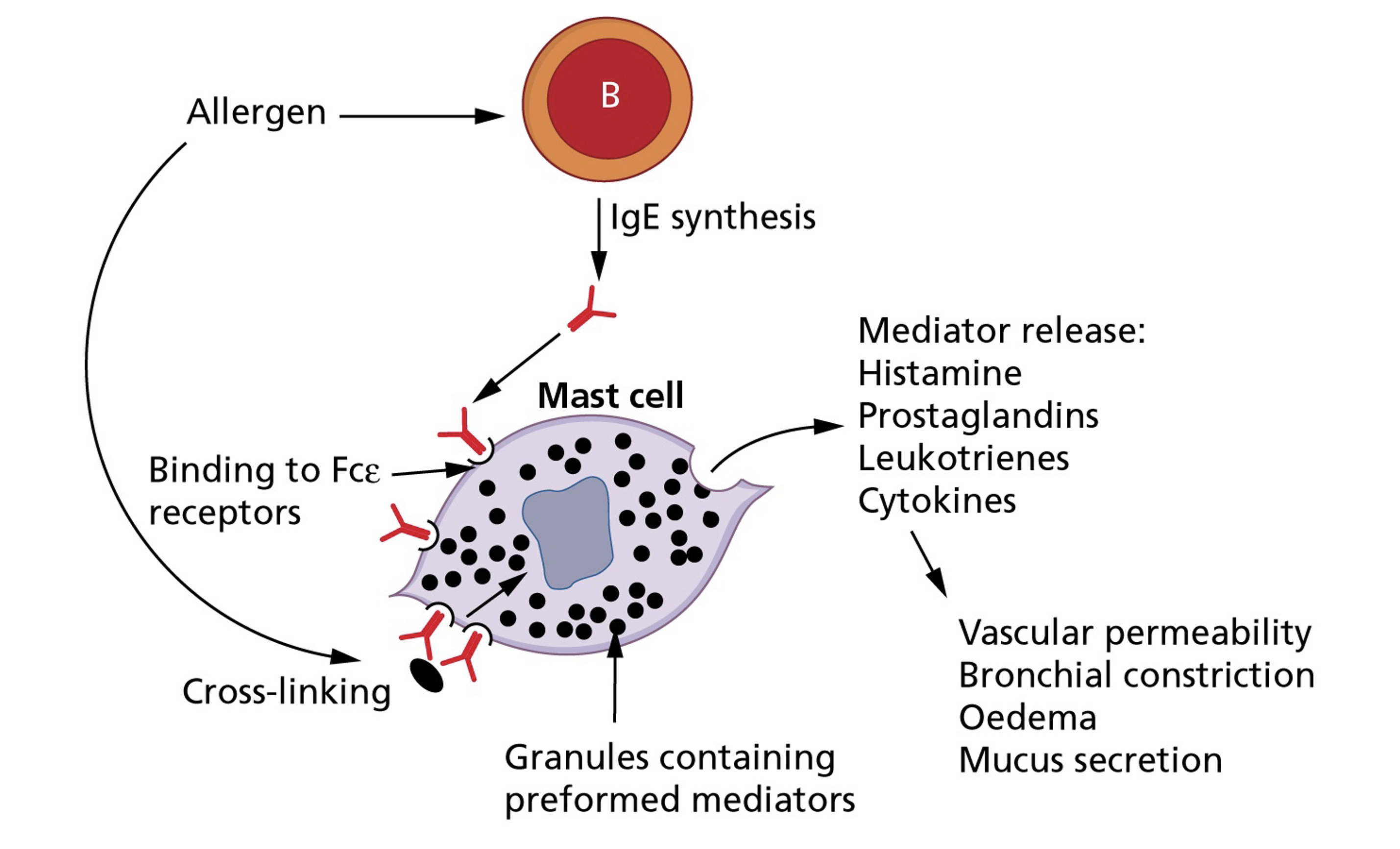
Cell-mediated immunity-1
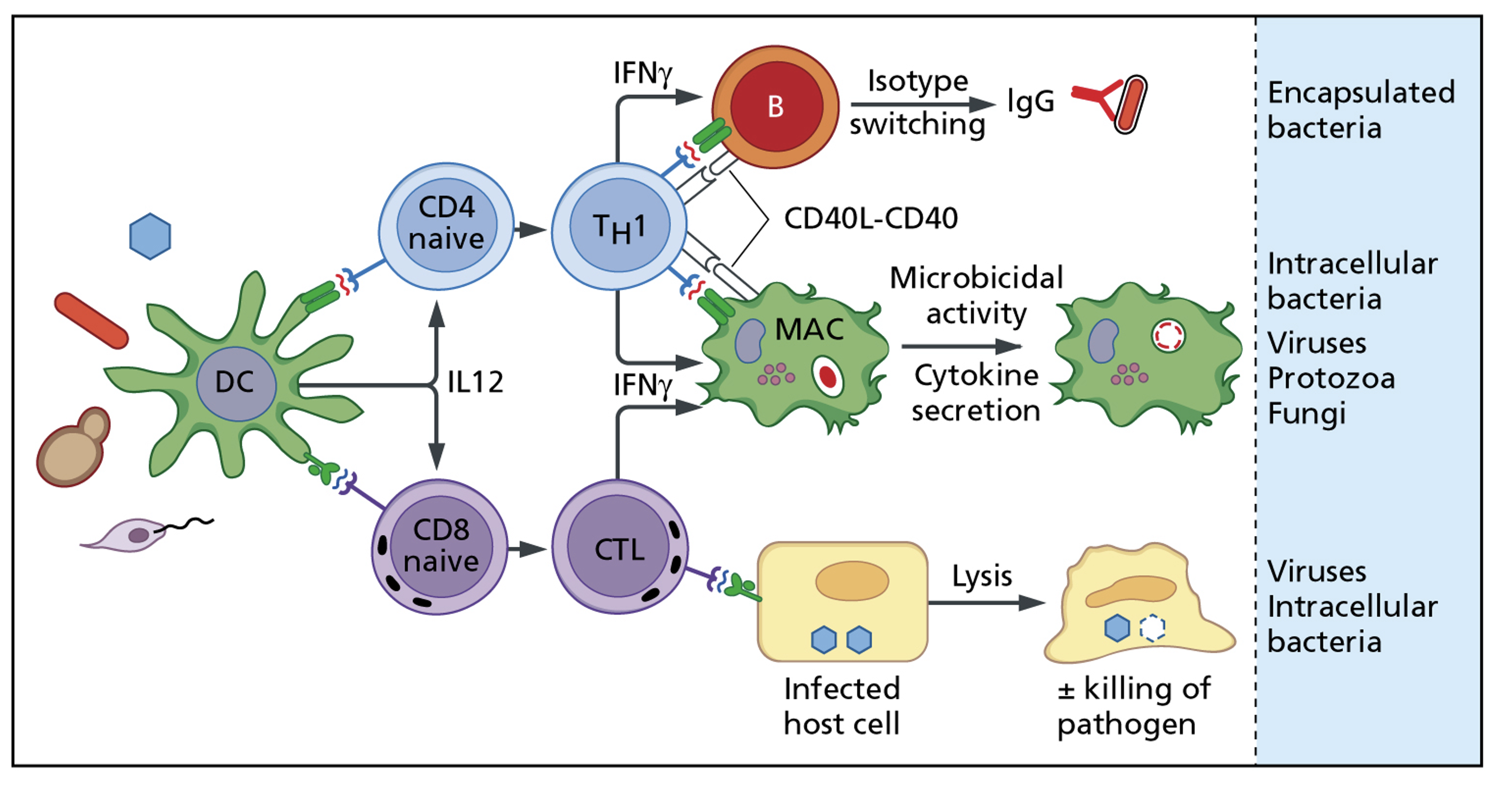
Cell-mediated immunity-2
Cell-mediated immunity-Drug allergy
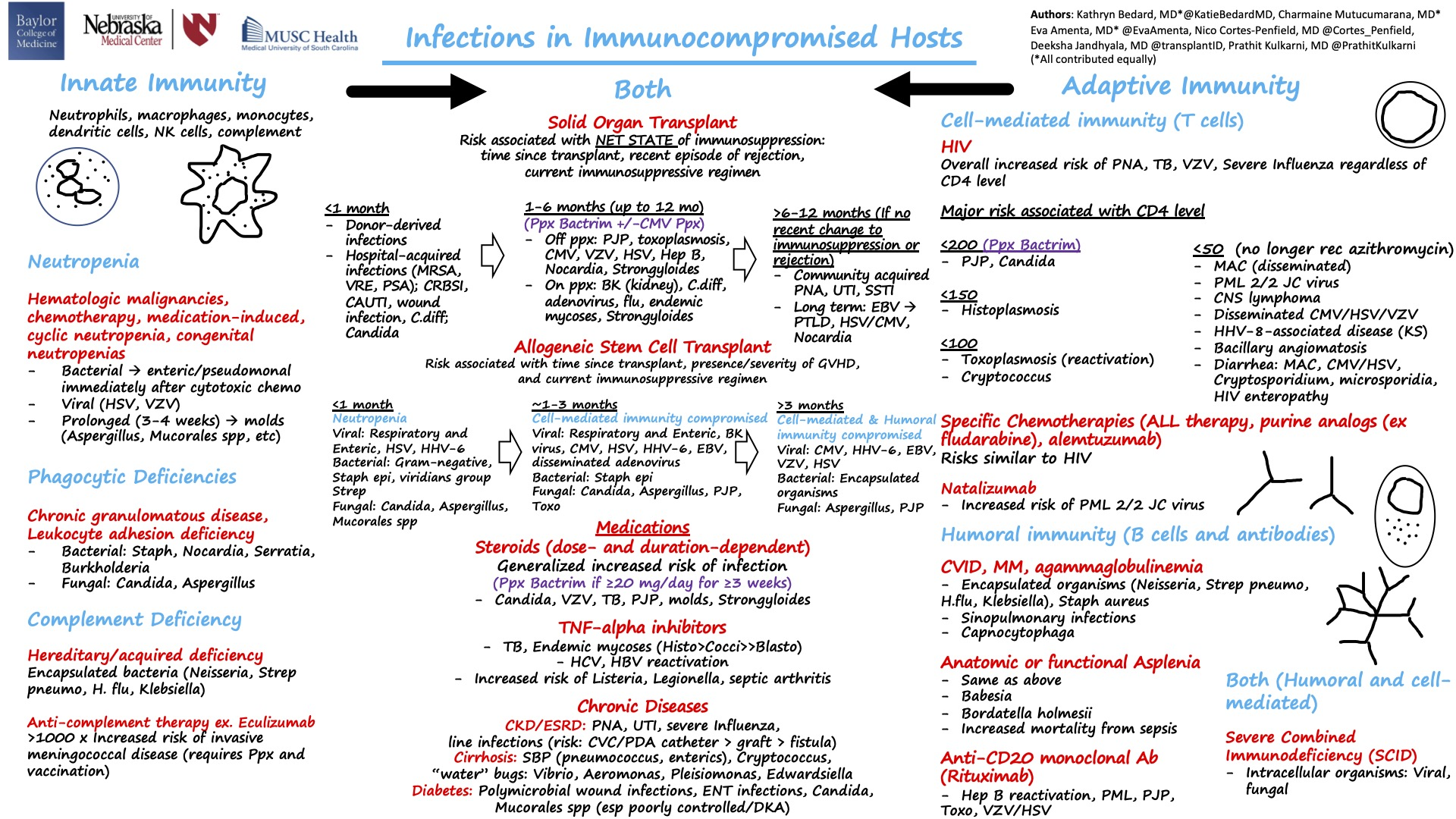
Infections in immunocompromised hosts
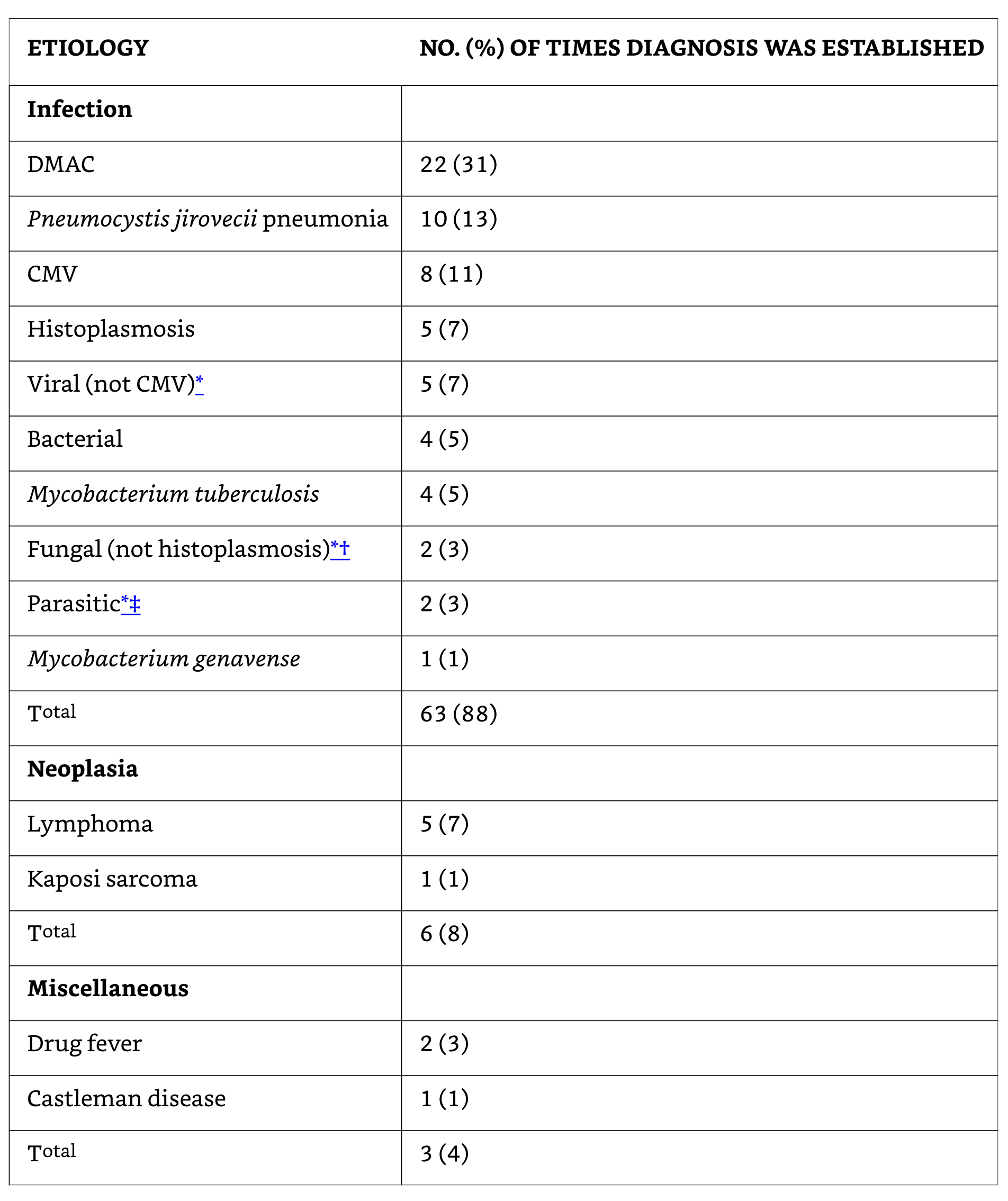
Etiology of fever in HIV-Associated FUO (n=70)
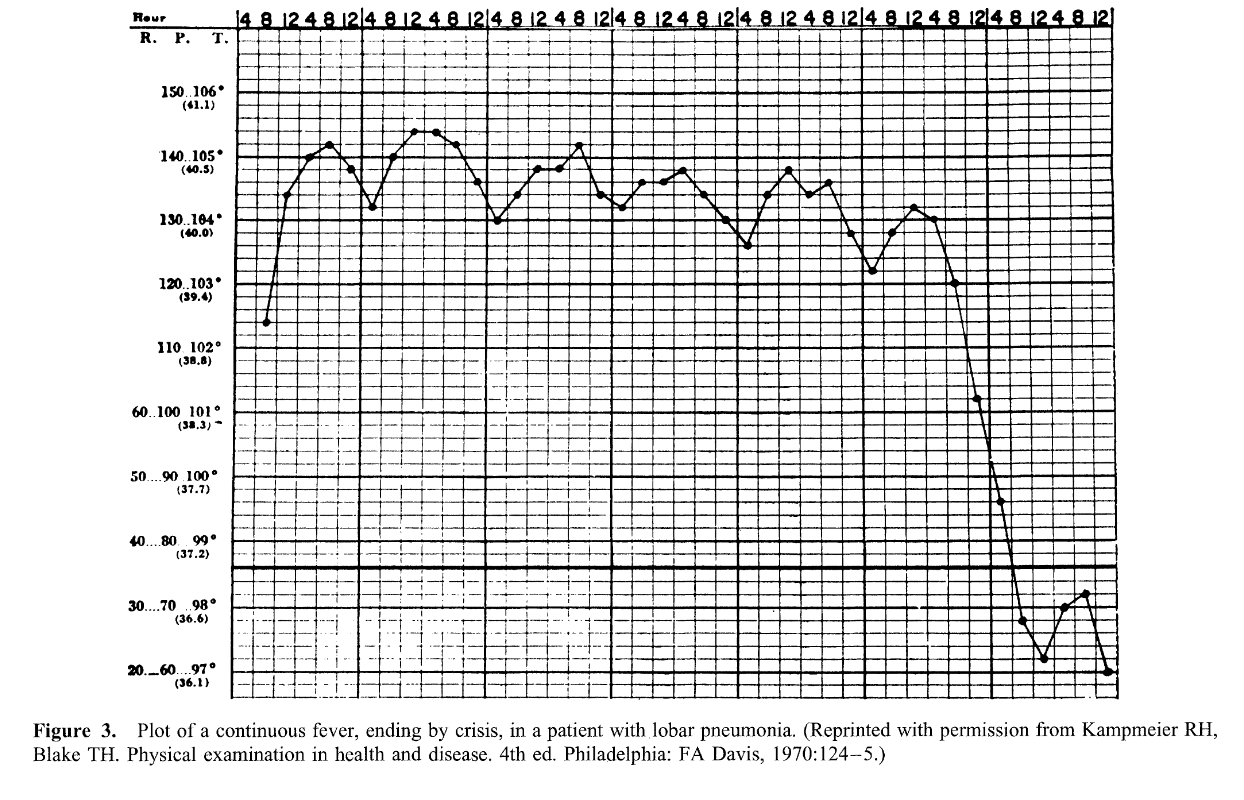
Continuous sustained fever
- Continuous (sustained) fever with slight remission not exceed 2°C
- Lobar and Gram negative pneumonia
- Rickettsiosis
- Typhoid fever
- CNS disorders
- Tularemia
- Falciparum (malignant tertian) malaria
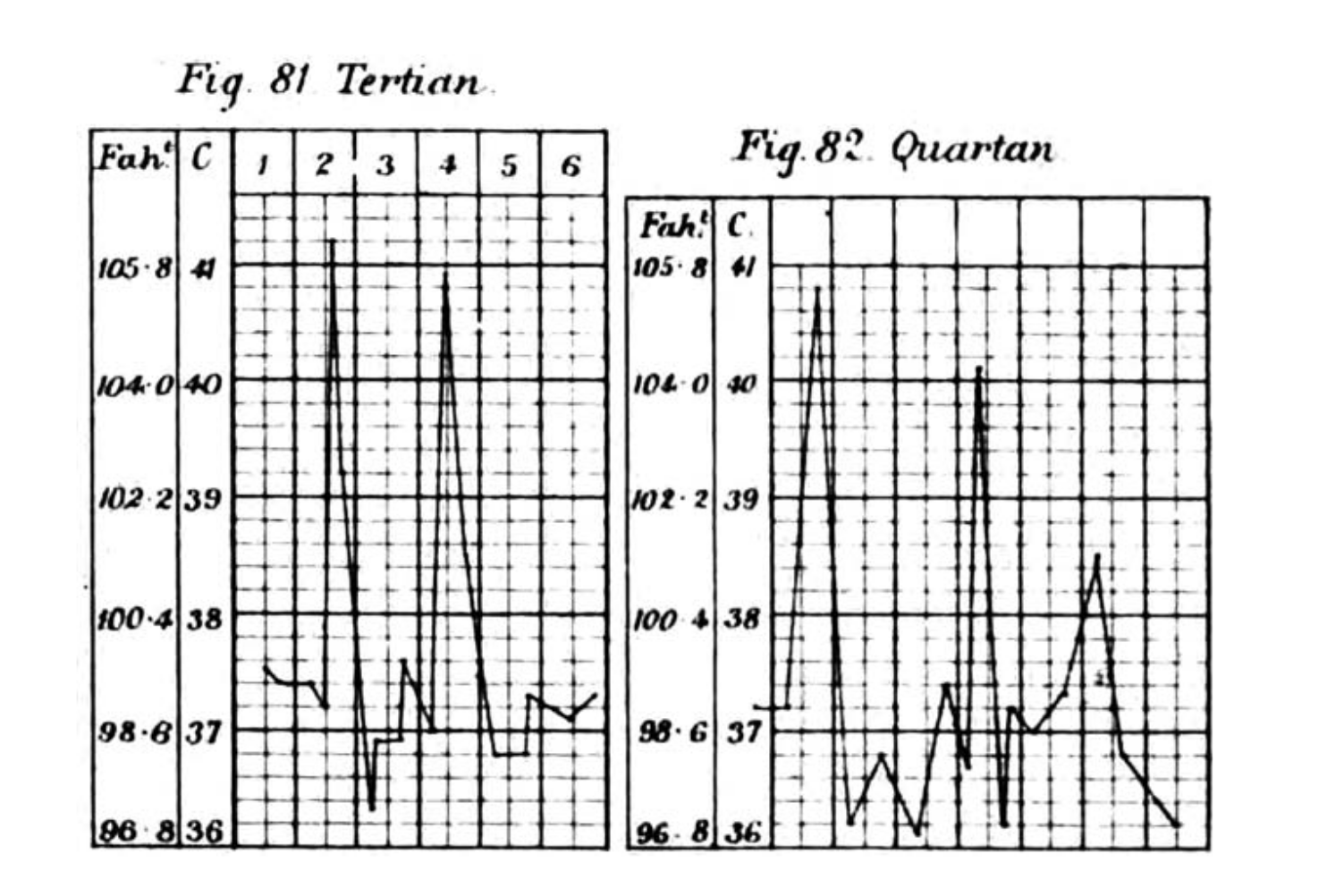
Malaria fever
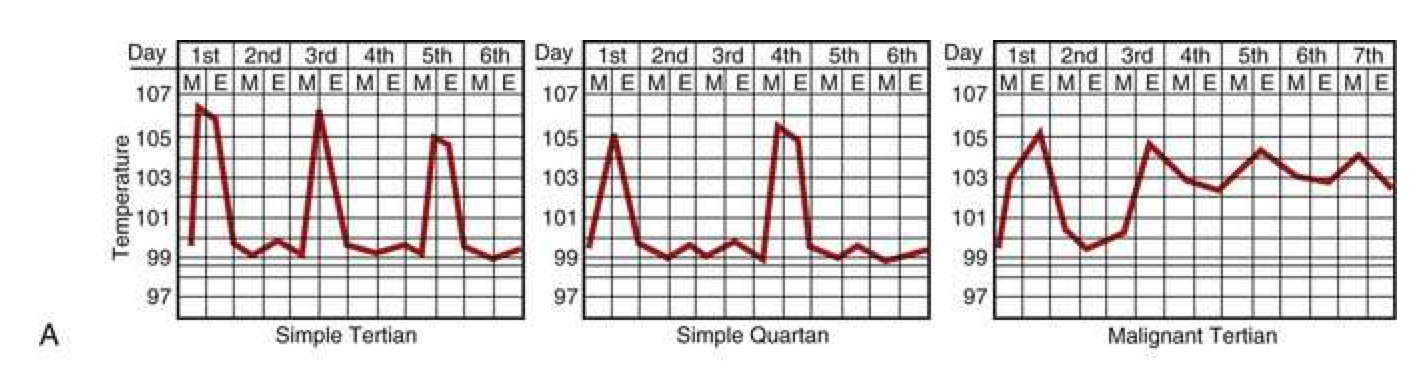
Febrile paroxysms may occur every other day for P. vivax, P. ovale, and P. falciparum and every third day for P. malariae. Paroxysms occurring at regular intervals are more common in the setting of infection due to P. vivax or P. ovale than P. falciparum. With improvements in early diagnosis and treatment, this traditional description of cyclic fever is seen infrequently.
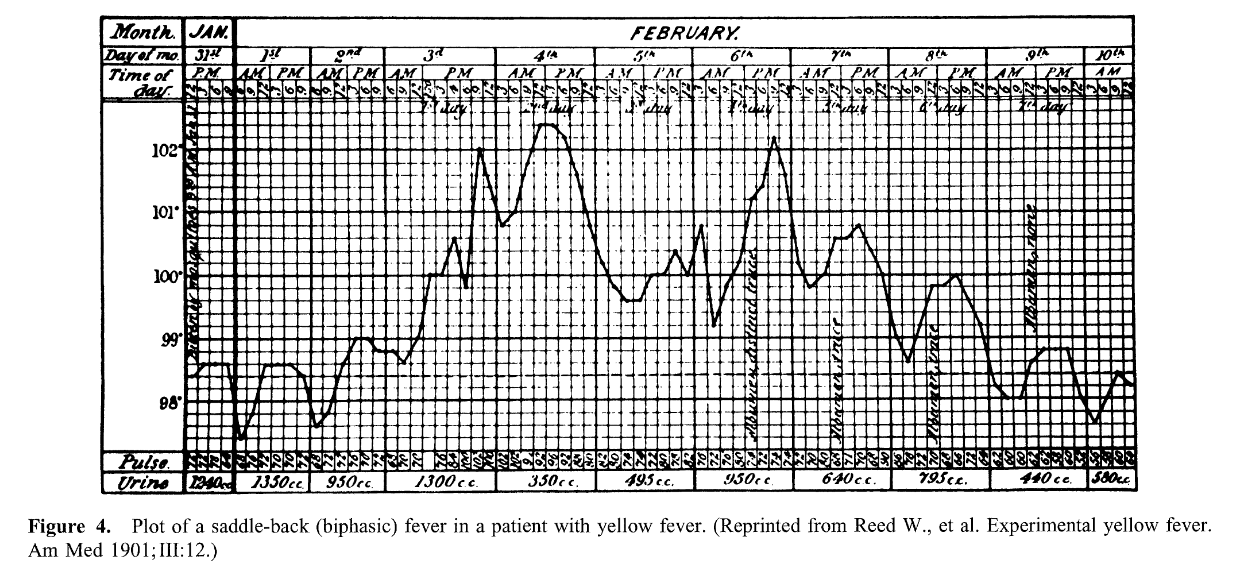
Saddle-back (biphasic)
- Several days of fever, distinct reduction in fever for ~ 1 day, and then several days of higher fever
- Dengue and yellow fever
- Colorado tick fever
- Rift valley Fever
- Influenzae and other viral infections
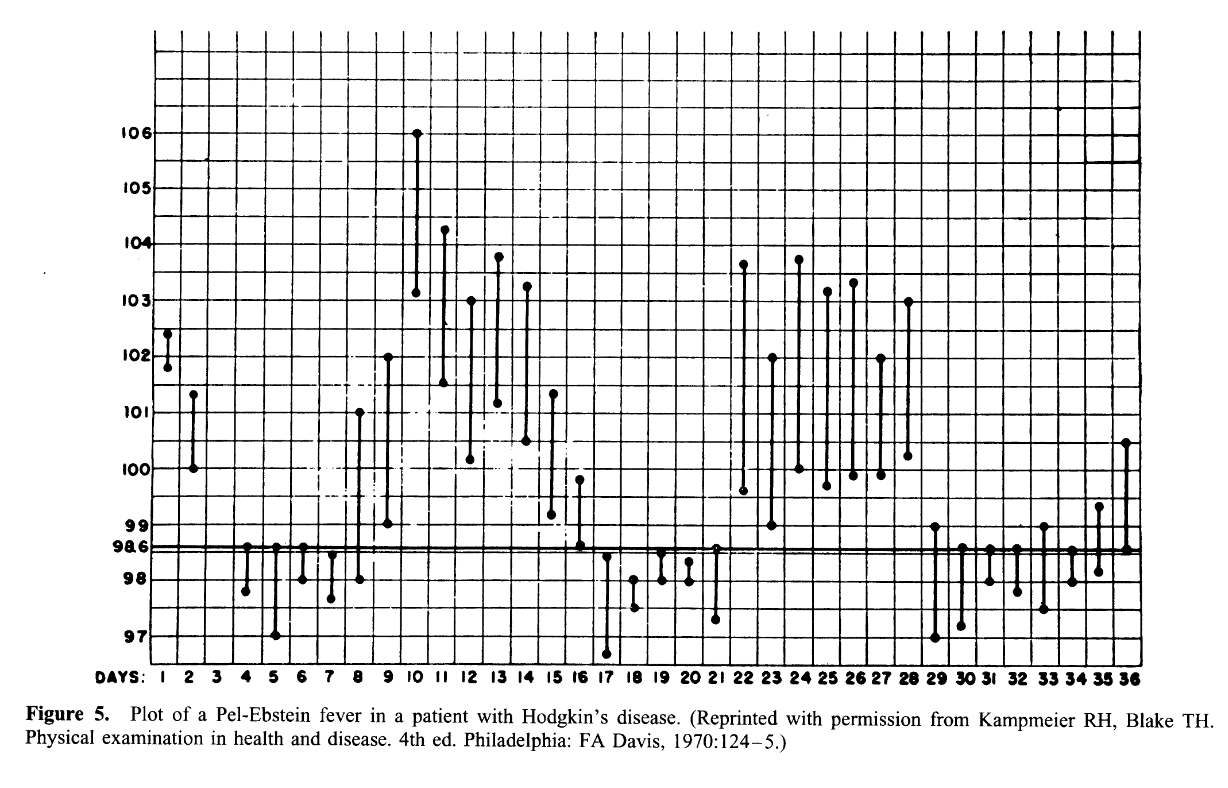
Pel-Ebstein fever
- Weekly or longer periods of fever and equally long afebrile periods, with repetition of the cycle
- Hodgkin’s disease
- Brucellosis due to Brucella melitensis
- Occasionally tuberculosis
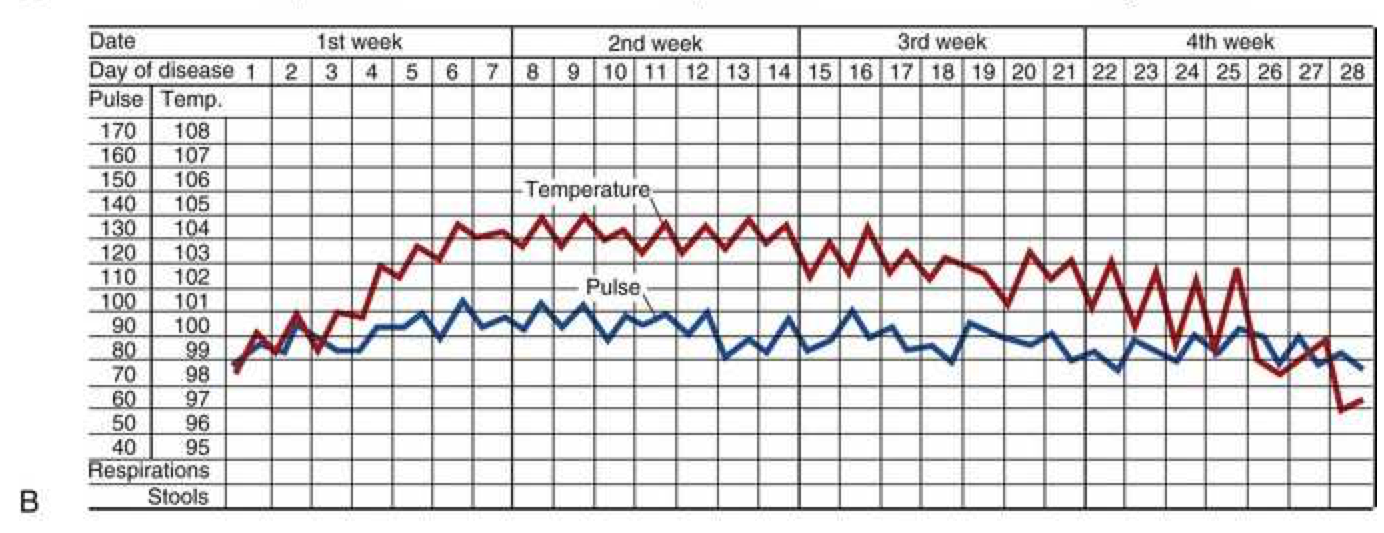
Typhoid fever
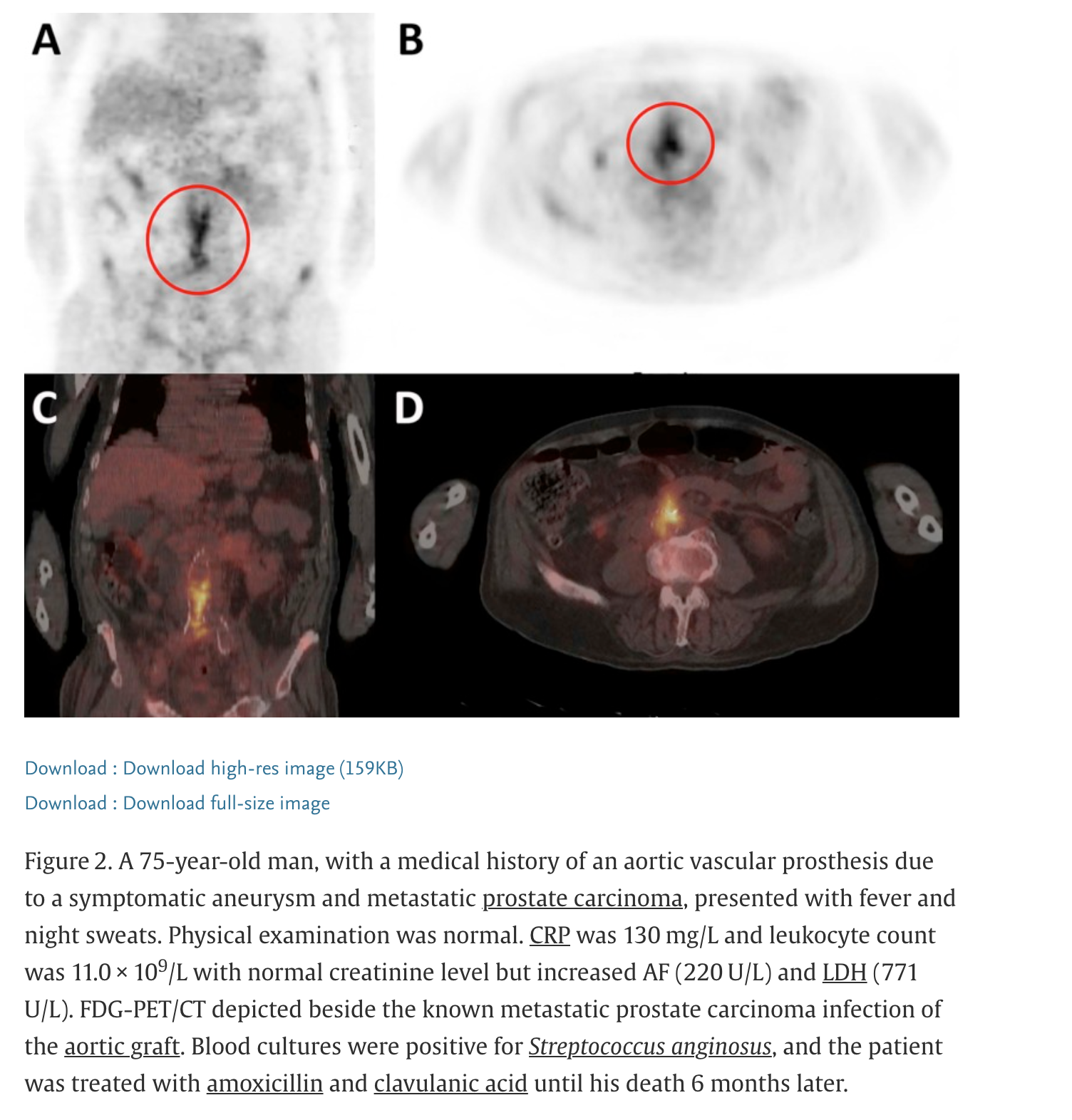
Physical examination
- Some signs are subtle and may require repeated exams to be appreciated
- Vigorous search for lymphadenopathy (consideration for biopsy)
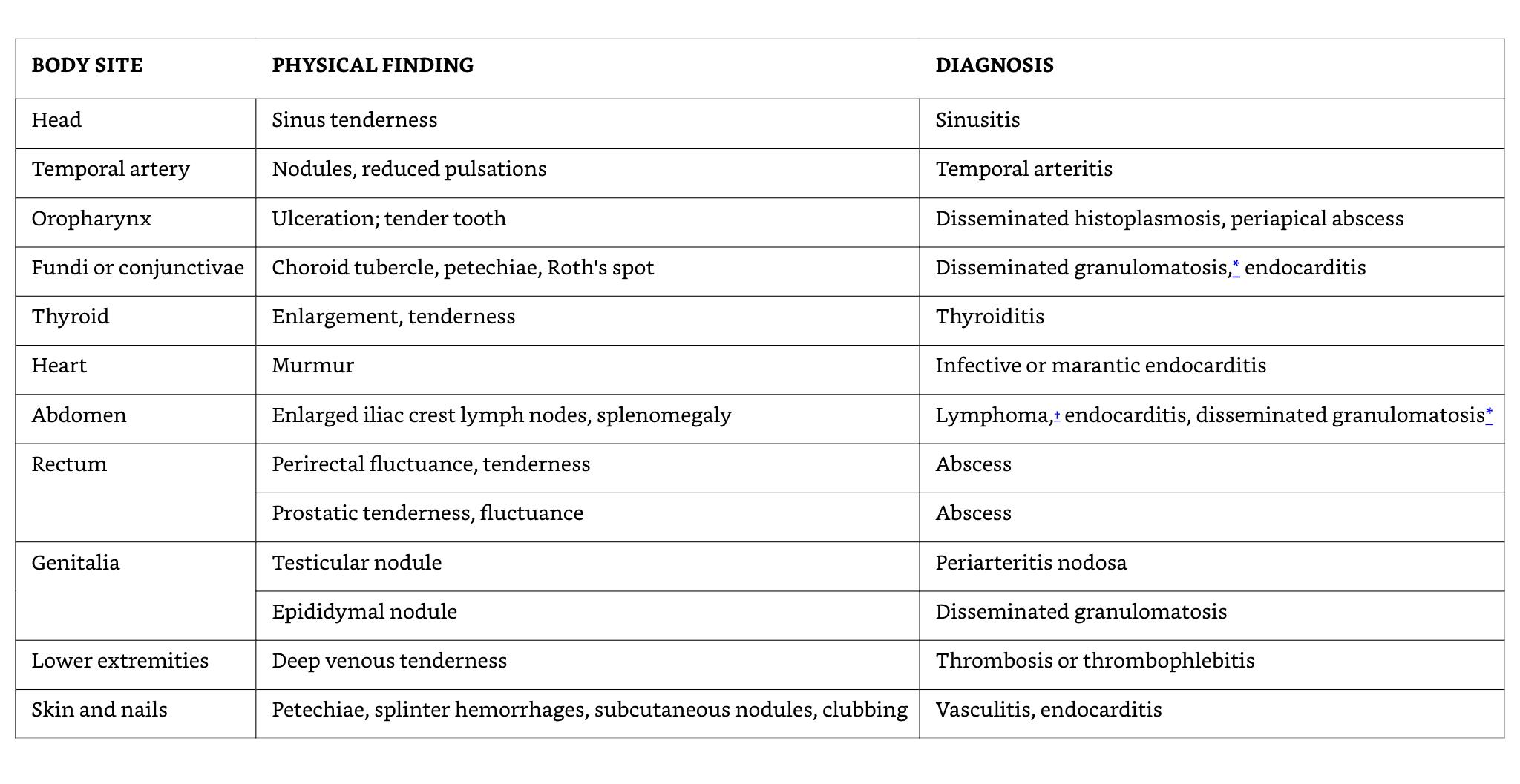
Examples of potential diagnostic clues

18F-fluorodeoxyglucose (FDG) positron emission tomography (PET)
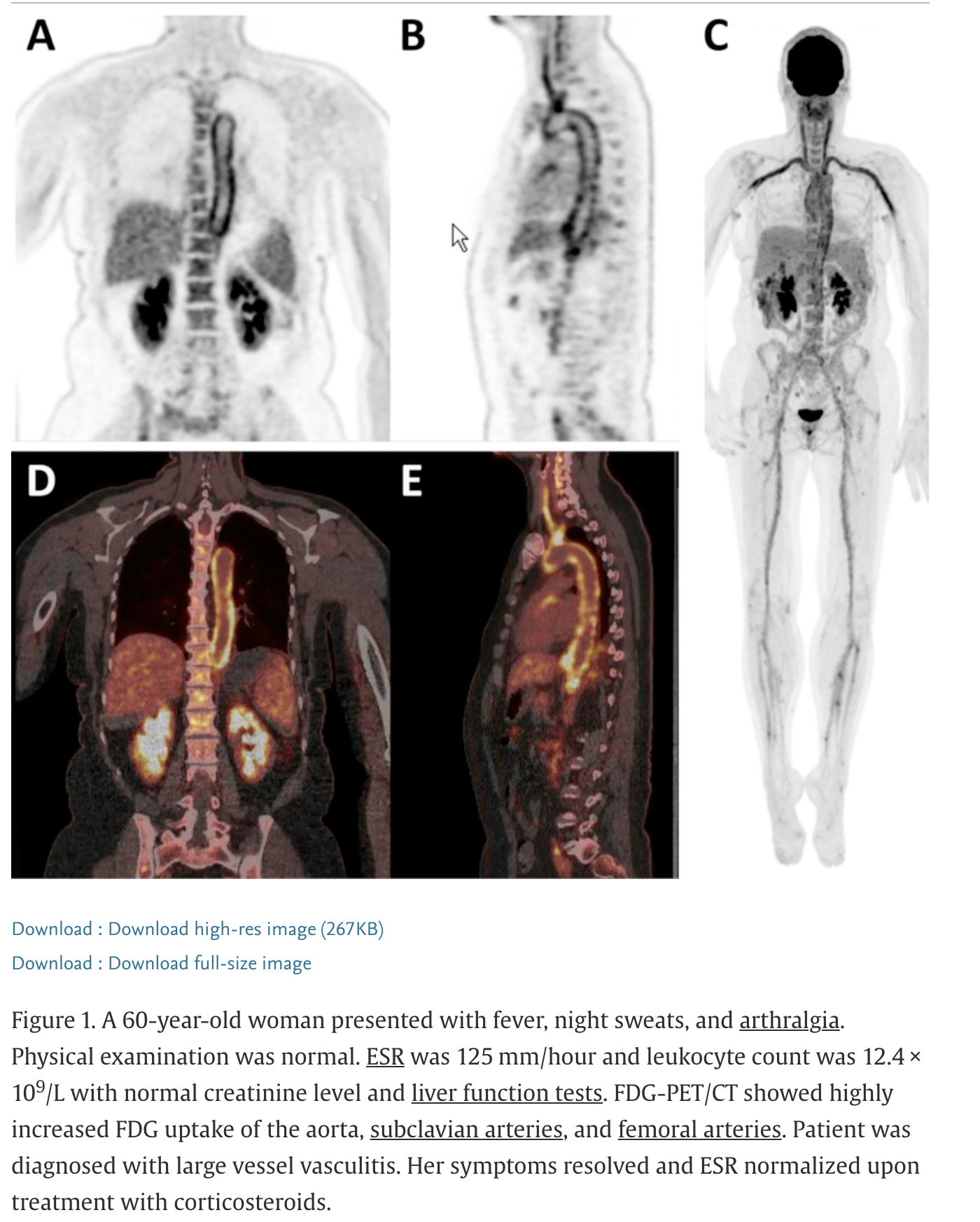
F-fluorodeoxyglucose (FDG) positron emission tomography (PET)
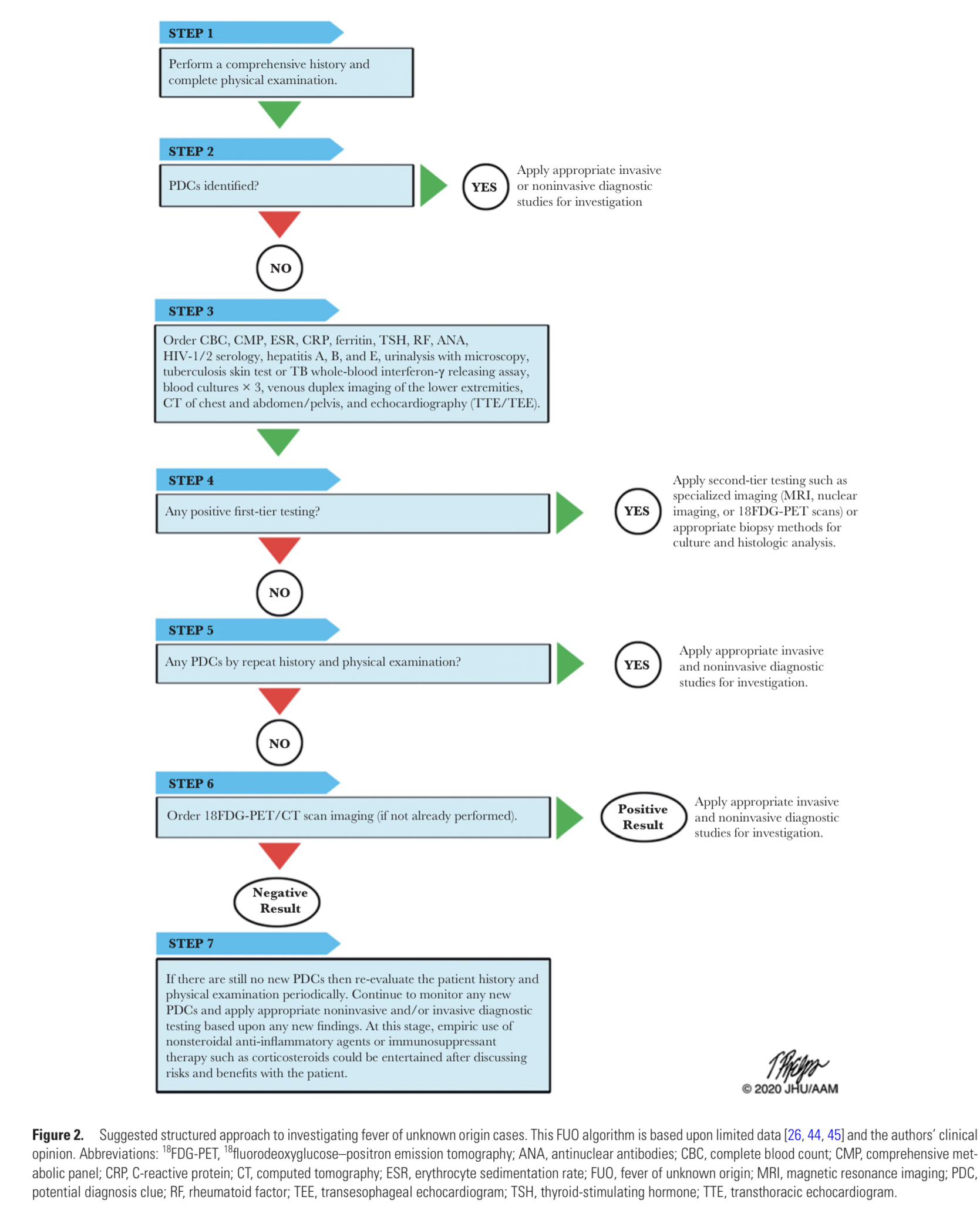
Diagnostic summary